How Does IVF Work?

If you’re wondering how IVF works, you’ve come to the right place. In Vitro Fertilization (IVF) is the most efficient and effective fertility treatment in that it results in the quickest time to pregnancy of any treatment or natural remedy. But it is a mysterious subject convoluted by acronyms and just downright complex science. In this article, we are going to explain everything you need to know about how IVF works, both the fertility issues it tackles as well as the process of how it handles them. Buckle up, here we go!
How Does IVF Work to Solve Key Fertility Issues
IVF works by controlling for, avoiding, or creating workarounds to a large number of issues that cause infertility in both men and women. We’re going to cover some of the biggest one’s here.
How Does IVF Work To Fix Tubal Infertility
Tubal infertility occurs when a blockage (or absence) of the fallopian tube prevents the egg and sperm from meeting – or subsequently traveling back down the tube and implanting in the uterus.
Amazingly, because IVF removes the eggs from the ovaries and transfers the already partially developed embryos directly into the uterus, IVF completely bypasses the fallopian tubes. This allows those with damaged, severed, or even missing fallopian tubes the ability to get pregnant with IVF. In fact, if damage to the fallopian tubes is severe enough, your reproductive endocrinologist may even suggest removing them before preceding to In Vitro Fertilization.
How Does IVF Work To Fix Ovulatory Issues
Well, this is actually quite simple. In IVF, the eggs are removed from the ovaries before ovulation even occurs. While people undergoing IVF take a “trigger” shot/medication designed to finalize egg maturation and induce ovulation, it’s critical that the egg retrieval takes place before the eggs are actually ovulated.
If the eggs are indeed released from the ovaries – the IVF cycle is a bust and must be canceled. Fortunately, this is exceedingly rare because patients are monitored closely and given medications to prevent premature ovulation.
How Does IVF Work To Fix Sperm Quality and Quantity Issues:
Men are the sole cause of or partially responsible for approximately 33% and 50% of infertility cases, respectively. While sperm health is a complex issue that has many causes (some of which can be improved naturally or with medications), IVF itself is a very effective workaround for many of these issues and can be combined with other treatments for certain severe cases.
Because sperm are placed in very close proximity with an egg in conventional IVF or injected directly into the egg with Intracytoplasmic sperm injection (ICSI), a man simply does not need to have sperm capable of making the arduous journey through the female reproductive tract.
For cases of male infertility in which the man has no sperm in their ejaculate, IVF can be paired with sperm extraction/retrieval procedures (PESA, TESA, TESE) to physically remove sperm from within the male reproductive tract. This may sound crazy, but men often produce sperm without it ever getting mixed in with the semen that is ejaculated due to congenital abnormalities or other blockages. Before deciding on a sperm extraction procedure, a man’s FSH is usually tested to determine if sperm may be present or not.
Sperm extractions can not be paired with Intrauterine Insemination or other treatments as the number of sperm retrieved during these procedures is far to low to effectively be paired with less effective treatments.

How Does IVF Work To Fix Egg Quality Issues:
While the extent IVF works to fix egg quality issues is somewhat controversial (and some will still need donor eggs), IVF can improve egg quality – in both direct and indirect ways.
Direct Improvements to Egg Quality
The main utility of IVF is that it “saves” eggs. Normally a woman recruits (or begins to develop) approximately 1,000 eggs each month but only 1-2 survive, fully develop, and are ovulated. IVF “saves” a portion of these eggs by developing and maturing a larger number of these eggs – possibly even more than 50 eggs (though that is quite rare and typically only seen in younger women if at all).
Another way to put this fact of IVF growing more eggs – is that it matures or improves the quality/viability of many eggs. A mature egg means a higher quality egg.
Similarly, not every egg is genetically normal. So, by producing more eggs each month, you are in a very real way improving the odds that a genetically normal egg will be developed that month.
Indirect Improvements to Egg Quality
During IVF, eggs develop in a highly controlled environment. People often know when their IVF cycle will start months in advance. And that’s a good thing. Dietary changes, supplements, as well as numerous medications have been shown to improve egg quality – especially when taken for a full 90 days before the IVF cycle (the final stages of egg development take approximately 90 days).
Uterine Issues
Generally speaking, there are two types of uterine problems. Physical/structural issues and lining issues. IVF certainly doesn’t help structural issues with the uterus – these often need to be corrected surgically before IVF. Still, many medications (estrogen, progesterone, and even things like aspirin, hCG, Lovenox, and Platelet Rich Plasma PRP) taken during IVF help ensure the uterine lining is appropriately developed and receptive to an incoming embryo.
That said, the medications taken to stimulate the ovaries often interfere with uterine receptivity. Because of this, people often split the IVF procedure into two separate cycles – one for ovarian stimulation and egg retrieval, the other for uterine lining preparation, and a frozen embryo transfer. This allows hormone levels to level out and the uterine lining to be truly optimized before the embryo transfer.
Miscarriage
While it is still slightly controversial whether or not IVF can reduce the odds of miscarriage, there is certainly evidence that suggests it does – particularly in women over 35, those with autoimmune issues (diagnosed or undiagnosed), or those with known genetic disorders.
Generally speaking, there are two ways in which IVF may reduce the odds of miscarriage.
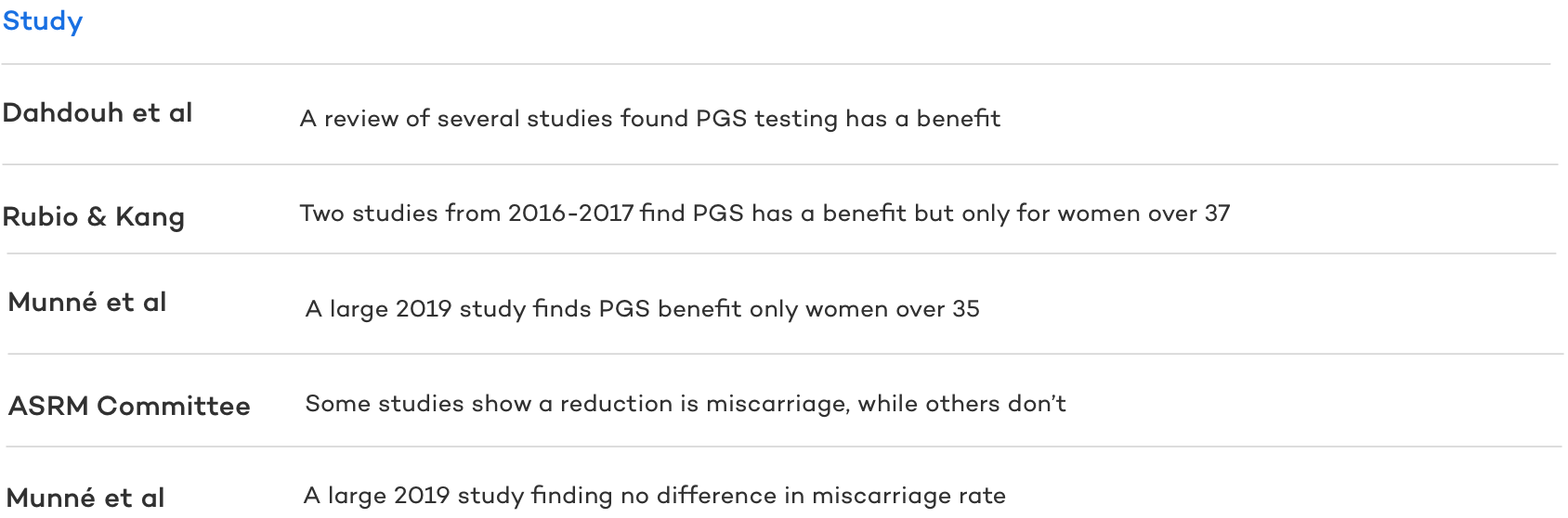
Preimplantation Genetic Testing (PGT)
Also known as PGS, PGT involves taking a small biopsy from a blastocyst embryo’s trophectoderm (the cells that will become the placenta) and running a genetic analysis on said embryonic cells. While the jury is still out , many studies show it can reduce the odds of miscarriage by detecting embryos with chromosomal abnormalities (aneuploidy) and only transferring normal (euploid) embryos.
Reproductive Immunology
IVF itself doesn’t itself treat inflammatory and immunological issues causing infertility or recurrent pregnancy loss. Still, because IVF offers the most control, it allows for many immunological medications to be prescribed at the proper time to assist with conception and pregnancy.
While reproductive immunology can be combined with other treatments (for example – IUI or Donor Egg IVF) it is most often used with IVF for the treatment of recurrent pregnancy loss and repetitive IVF implantation failure.
There remains controversy amongst fertility specialists regarding therapies for immune system modulation. Still, CNY doctors are amongst the leading reproductive immunologists and often use immunological protocols when they have clinical reasoning to suggest it will lead to the highest chance of success.
Elective
It may come as a surprise to some, but people often do IVF for elective reasons. The two most common elective reasons for pursuing IVF are sex/gender selection and reciprocal IVF.
Sex Selection
Commonly referred to as gender selection or family balancing, sex selection uses PGT-A (PGS) genetic testing to look at the chromosomes inside of IVF embryos and transfer an embryo that has the desired biological sex.
Reciprocal IVF
Reciprocal IVF is done by lesbian (and trans men) couples as a way of having both parents intimately and biologically involved in the child creation process. In reciprocal IVF, one partner’s eggs are used to make the embryos, which are then put inside the other partner’s uterus.

How Does IVF Work: A Step by Step Guide to the IVF Process
In basic terms, IVF removes eggs from the mother to be (or donor), fertilizes them in a lab, and then places said fertilized eggs back into the woman’s uterus. Of course, there are a host of variations like INVOcell (which uses a small plastic device and the woman’s vagina as a replacement to the embryology lab), Mini IVF (really just a marketing term to describe IVF with less medications) as well as those which use donor eggs, sperm or gestational carriers.
For the sake of simplicity, however, let’s focus here on a relatively standard IVF process which can be broken down into four main steps:
- Ovarian Stimulation
- The Egg Retrieval
- The Embryology/IVF Laboratory
- The Embryo Transfer
Ovarian Stimulation
Ovarian stimulation is the phase of the IVF process in which exactly what it sounds like happens, does. During ovarian stimulation, women take injectable medications (namely FSH and LH) that tell the ovaries to grow and develop many eggs to maturity (as opposed to the one that is normally selected to fully develop). The premise of ovarian stimulation is simple. Not every follicle is an egg. Not every egg is mature. Not every mature egg is fertilized. Not every fertilized egg (embryo) develops. Not ever embryo results in a successful transfer. Not every successful transfer results in a live birth. Because of this, we ideally want a good number of eggs. FSH helps achieve this goal.
The number of eggs a woman produces is based on several factors, including:
- the medication dose – a low dose protocols generally produces fewer eggs; higher doses produce more eggs. However, there are some populations often referred to as “poor responders” who develop a similar number of eggs regardless of the medication dose.
- The woman’s age and ovarian reserve – generally older women and those with low ovarian reserve produce fewer eggs for any given medication dose.
- Weight – which may influence how the body processes the medications.
- previous response to medications (usually the best indicator of a future response)
- other fertility and medical concerns
Ovarian stimulation typically lasts for around ten days, starting on days 2-4 of a woman’s menstrual cycle. During this period of daily injections, the patient will be followed closely with monitoring appointments every few days to ensure safety, an appropriate response to medications, and, if necessary, adjust the dosage of medications.
After the follicles reach an appropriate size, the trigger shot is taken to finalize egg development.
How do IVF injections work?
The growth of eggs and their release from the ovaries are influenced by two hormones from the pituitary gland: Follicle Stimulating Hormone (FSH) and Luteinizing Hormone (LH) – known collectively as gonadotropins.
In a natural (non medicated cycle), FSH is regulated by the hypothalamic-pituitary-gonadal axis, part of the endocrine system (hence the name of the fertility doctor – reproductive endocrinologist). The production and release of FSH is determined by circulating blood levels of certain hormones:
- At the onset of a woman’s menstrual cycle, hormone levels (estrogen in particular) are low.
- The hypothalamus senses these levels and releases gonadotrophin-releasing hormone (GnRH) from the hypothalamus in the brain
- GnRH then travels and binds to the anterior pituitary gland at the base of the brain.
- The binding of GnRH to the anterior pituitary causes the synthesis and release of FSH and LH – which are then carried to through the bloodstream where the hormones bind to receptors in the ovaries.
- The binding of FSH to the ovaries causes follicular/ovarian growth.
- With this growth, the follicles produce more and more estradiol and inhibin, which slows the release of GnRH and thus FSH. But as more estrogen is produced from the developing follicles, it stimulates a surge in FSH and LH, which stimulates ovulation.
As you see, FSH’s binding to the ovary is the key driver of follicular growth. But natural levels of FSH can only do so much. By injecting FSH directly into the body during the stimulation phase of IVF, the ovaries are bombarded with FSH and thus develop an unnaturally large number of follicles and eggs.
The Egg Retrieval
The egg retrieval is easily the most surgically invasive part of the IVF process. In fact, it’s really the only part of IVF that can be classified as a surgery. The egg retrieval is relatively quick, taking only 5-15 minutes, and there are no incisions or stitches placed afterwords. It can be thought of as a “blood draw” taken from the follicles through the vagina (only follicular fluid is collected instead of blood).
During the egg retrieval itself, you shouldn’t feel or remember a thing thanks to the anesthesia. Fortunately, due to the relatively mild nature of the egg retrieval, the type of anesthesia used doesn’t require intubation making for an easier process and recovery.
How The Egg Retrieval Works?
Once you are sedated, the doctors will use an ultrasound-guided probe to locate the ovarian follicles (which house the eggs). Then using a hollow needle with suction capabilities attached to the ultrasound, the physician will pierce through the vaginal wall and into the follicle. The follicle is filled with follicular fluid, which should contain an egg. The physician will then turn on the suction, draining the follicular fluid and collecting it in labeled test tubes. These test tubes are then brought immediately to the IVF/Embryology Laboratory.
Once the physician has drained every follicle on each ovary, the anesthesiologist will bring you out of sedation. You will likely be transported to a nearby recovery room where you will continue to be monitored by the clinical nursing team. It usually takes 5 to 10 minutes to come out of sedation and another 30 minutes to fully come around. At this point, you will likely be free to go home (of course, you yourself will not be allowed to drive).
The IVF Laboratory
Once inside the IVF lab, one of the embryologists will look through the follicular fluid to locate and isolate any eggs – placing them in a nourishing media where they will continue to develop for a few hours prior to freezing or fertilization. This culture media is designed to have the proper pH and nutrients needed for fertilization by mimicking the natural environment of the Fallopian tubes.
Approximately 4 hours after the egg retrieval, the eggs have fully matured and ready to be fertilized.
How IVF Fertilization Works
Generally speaking, there are two types of IVF Fertilization:
- Conventional: In conventional fertilization, the embryologist adds sperm directly to the culture dish containing the eggs. The sperm attach to the shell of the egg (the zona) and penetrate it for fertilization. Because the sperm and egg are already in relatively close proximity, this can work for a large number of people, including those with mild male factor infertility.
- ICSI: With ICSI fertilization, a motile sperm is singled out using a microscope. Its tail is then carefully damaged by the embryologist in order to activate the sperm to prime it for fertilization. The embryologist then sucks that sperm into an incredibly small hollow needle and then injects the sperm directly into the egg. This is generally highly recommended (or required) for those with severe male factor infertility but widely practiced in many clinics (including CNY) regardless of any male factors.
How IVF Embryo Development Works
Following fertilization – the newly fertilized embryos are placed inside an incubator and serve as the “artificial uterus.” Maintaining a proper environment that mimics the Fallopian tube/uterus is absolutely critical to embryo development. Compared to normal air we breathe (78% Nitrogen, 22% Oxygen, less than 0.1% Carbon Dioxide), the incubators are connected to gas lines that maintain 88% Nitrogen, 5% Oxygen, and 7% Carbon Dioxide levels. This high level of carbon dioxide is needed to maintain the perfect pH in the culture media for embryo development. Low levels of oxygen are also needed to improve embryo development in culture. The incubators must be kept at body temperature (37 degrees Celsius) and at 100% humidity.
Embryos develop inside these incubators for up to 7 days until they reach the cleavage or blastocyst stage of development.
The Embryo Transfer
The embryo transfer is the final step of the IVF process. It is rather straight forward and works similarly to how you are already likely imagining. While the timing of the embryo transfer can vary greatly depending on if one is doing a fresh transfer in the same cycle as the egg retrieval or a Frozen Embryo Transfer (FET) sometime later, the process of the transfer itself remains quite similar.
While the woman is getting situated in the transfer room similar to an OBGYN exam, an embryo is loaded into a special transfer catheter syringe by an embryologist. The doctor and embryologist will then ensure your identity to make sure it matches the information labeled on the embryo.
Around this time, a speculum is placed into the vagina, which will allow the cervix to be visualized and cleaned. The catheter containing the embryo is then passed through the cervix and into the uterus using an ultrasound for guidance. Once in place, the embryo is expelled from the catheter onto the uterine lining.
The catheter is then given back to the embryologist where they will examine the catheter under a microscope to ensure the embryo has been properly expelled.
With the transfer complete, the patient is usually allowed to rest for about 15 minutes. During this time, the patient should be given follow-up instructions and scheduled for bloodwork 4-7 days and ten days post transfer.
The Bottom Line
IVF is a mysterious and complex process that works in a variety of ways to tackle both small and large issues preventing reproduction. While the ways in which IVF tackles each issue causing infertility may be different – it is indeed a medical marvel just how many issues IVF tackles.
Of course, any decision to pursue IVF (or other less effective treatments like IUI -aka artificial insemination) should be made after male and female fertility testing with the consultation of a trained fertility specialist. Here at CNY, we consult with and treat clients from around the globe. People seek out our experts for our unique expertise and unique approach, which allows for most treatments to be done for 1/3 to 1/2 the cost of the national average. Because of this, over half our clients travel to us from states with no CNY Fertility office through our user-friendly travel program. No matter where you live, we can help you decide if IVF will work for your family-building needs.