Embryo Transfer: What It Is, What to Expect, The Different Types, and More
The embryo transfer is one of the most important steps in an IVF cycle. It is the moment when an embryo, created in the lab, is carefully placed into the uterus with the hope that it will implant and grow into a healthy pregnancy.
While the procedure itself is simple and usually quick, there are many details that patients want to understand before reaching this stage.
In this article, we will explain what an embryo transfer is, what to expect during the process, the different types of transfers, and other key information to help you feel prepared and informed.
Fast Facts About Embryo Transfers:
- An embryo transfer is the final stage in the In Vitro Fertilization (IVF) process, where the fertilized egg—now an embryo—is placed in the woman’s uterus.
- The embryo is loaded into a catheter, which is passed through the vagina and cervix and into the uterus where it is deposited.
- This generally takes place between 3 and 5 days after egg retrieval for a fresh transfer and anywhere from 4 weeks to several years later for a frozen transfer (FET).
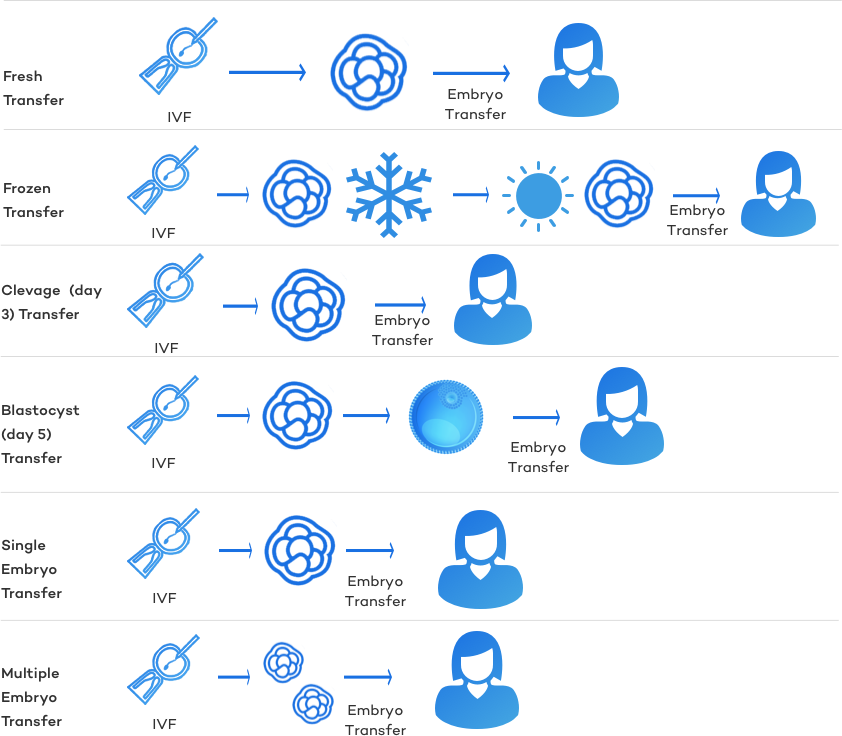
- There are many different types of embryo transfers: fresh, frozen, cleavage (day 3), blastocyst (day 5), single, and multiple embryo transfers.
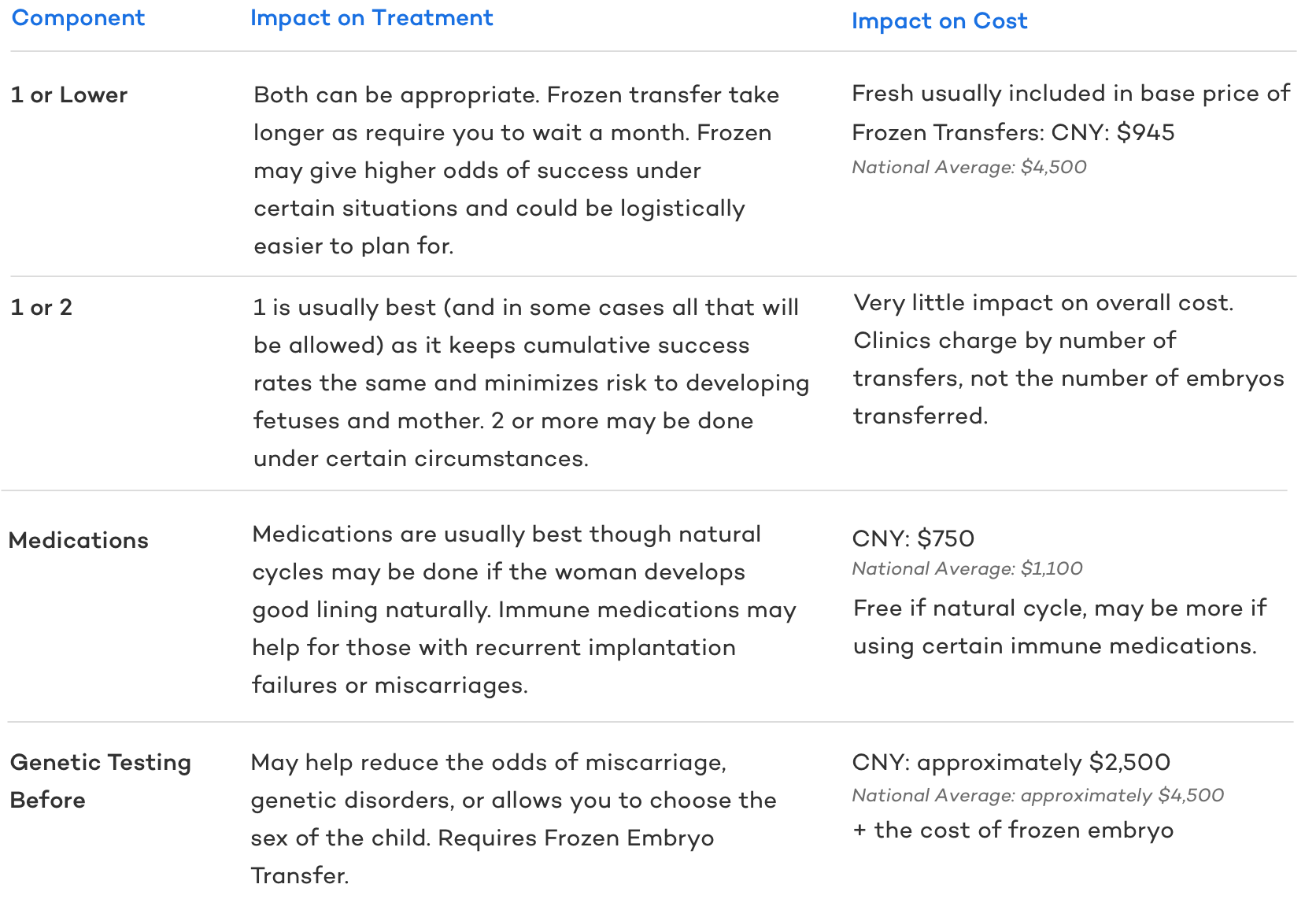
- Today, the standard practice is to transfer one embryo at a time, occasionally two. This approach lowers the risk of multiple pregnancies while maintaining the same overall live birth rates per retrieval. Any embryos not transferred are frozen for future use. If the first transfer is fresh, additional embryos are frozen afterward; if the first transfer is frozen, the remaining embryos stay stored as part of what is known as a freeze-all cycle.
- The cost of fresh embryo transfer is usually included as part of the base cost of an IVF cycle. Frozen Embryo Transfers (FETs) are rarely included in this price and cost an additional $4-5,000 on average across the USA, though the price varies widely by clinic.

What is an Embryo Transfer?
An embryo transfer is the final step in the IVF process. After fertilization, the embryo is allowed to grow for several days before being placed in the uterus, where the hope is that it will implant, develop into a fetus, and ultimately result in the birth of a healthy child.
The procedure involves loading the embryo into a thin catheter, which is carefully guided through the vagina and cervix into the uterus. Anesthesia is not typically required, although a mild sedative such as Valium may sometimes be used.
Types of Embryo Transfer:
There are many “types” of embryo transfers, though the basic principle remains the same.
Fresh Embryo Transfer
Just as the term implies, a fresh embryo transfer is the transfer of (an) embryo(s) that has not been frozen.
Frozen Embryo Transfer (FET)
A Frozen Embryo Transfer is a cycle in which frozen embryos from a previous IVF or donor egg cycle are thawed and then transferred into a woman’s uterus.
A frozen embryo transfer may be done for a number of reasons:
Medically Advised Due to Uterine Receptivity: During an IVF cycle, a woman is in a state of controlled ovarian hyperstimulation. This can produce physiological stress on the woman’s body.
In some situations, the uterus may not be optimally prepared to receive an embryo at the same time. If the patient develops ovarian hyperstimulation syndrome, has elevated progesterone or estrogen levels, or if the uterine lining measures less than 7 mm at the time of trigger, a “freeze-all” approach may be recommended.
In this case, all embryos are frozen and transferred later in a frozen embryo transfer (FET), when the uterine lining is more receptive and the chances of implantation are higher.
A Second Embryo Transfer: In a conventional IVF cycle, it is common for 10-15 eggs to be produced through controlled hyperstimulation, which results in a number of high-quality embryos available for transfer.
Today’s standard practice is to transfer one (sometimes two) embryos into the woman’s uterus and freeze all remaining embryos to increase the chance of future pregnancy. The remaining embryos are available if the couple wants to continue expanding their family after giving birth or if the first transfer fails.
Easier to plan: Because there are times when it is medically advised to convert a fresh cycle to a freeze-all cycle with an FET, many, particularly travel clients, find it much easier to plan in advance for a frozen transfer. FETs are rarely ever canceled, can be easily planned, and offer comparable success rates as a fresh transfer.
Cleavage (Day 3) Stage Embryo Transfer:
Cleavage-stage embryos are named for the fact that their cells are dividing, or cleaving, without the embryo itself increasing in size.
This stage is typically reached around day three, though it can occur as early as day two or as late as day four. For this reason, they are often referred to as “day three embryos.”
Some fertility specialists believe that the best environment for an embryo to develop is the uterus itself. Because not all embryos survive to day five, transferring at the cleavage stage can give the embryo a greater chance to continue developing in its natural environment.
At CNY, we generally recommend a day three transfer if there are fewer than four embryos on day one.
Blastocyst (Day 5) Stage Embryo Transfer
A blastocyst is an embryo that has developed into a single-layered sphere of cells encircling a fluid-filled cavity with a dense mass of cells grouped together.
Blastocysts contain anywhere from 60 to 120 cells. This usually occurs on day five but may happen on day 6, 7, or even 8.
By this stage, the embryo has differentiated into two cell types: the trophectoderm, the cells on the periphery of the embryo that form the placenta, and the inner cell mass (ICM), the dense mass of cells on the inside that forms the fetus if the embryo implants.
A blastocyst-stage embryo is often considered more favorable than an earlier-stage embryo because it carries a higher likelihood of being genetically normal, implanting successfully, and resulting in a live birth compared to a cleavage-stage embryo.
By allowing embryos to develop to the blastocyst stage before transfer, embryologists can more effectively identify and select those with the greatest potential for continued development.
An embryo that is grown to a blastocyst stage can also be genetically tested prior to transfer, which can help reduce the risk of miscarriage for some populations, avoid known genetic disorders, and select the sex of the child.
Single Embryo Transfer (SET or eSET)
A Single Embryo Transfer (SET) is the practice of transferring only one embryo into a woman’s uterus. This offers a reduced chance of multiples while maintaining a very similar rate of pregnancy.
Due to the reduced risk of an eSET along with having a very similar rate of pregnancy, eSET has quickly become the standard of practice for transferring embryos with an IVF procedure.
Multiple Embryo Transfer
A multiple embryo transfer is the placement of more than one embryo into the uterus during an IVF cycle.
While this is sometimes done, strict guidelines regulate the practice. Transferring too many embryos, or even more than one in certain situations, can pose significant risks and may place a clinic in violation of medical standards.
Summary of Embryo Transfer Types:
Some of the above-mentioned embryo transfers are mutually exclusive, while others could be classified together:
- Fresh Embryo Transfers and Frozen Embryo Transfers are mutually exclusive
- Cleavage Transfer vs. Blastocyst Transfers are mutually exclusive
- Single Embryo Transfer vs. Multiple Embryo Transfers are mutually exclusive
This means that a transfer could be a frozen single embryo blastocyst transfer, but it could not be a cleavage blastocyst transfer.
That said, IVF often results in many embryos, so you could do a Fresh Single Embryo Transfer followed by a Multiple Frozen Embryo Transfer months/years later from an embryo created in the same IVF cycle.
Key Decisions Regarding Embryo Transfers

When Does Embryo Transfer Occur?
The timing of an embryo transfer varies because every IVF cycle is unique and influenced by many closely monitored factors.
These factors determine the pace of each stage of treatment and ultimately set the timeline for transfer. Since the embryo transfer is the final step of an IVF cycle, the exact day can differ significantly from patient to patient.
For this reason, it is important not to become attached to a fixed calendar date or rigid timeline when preparing for your own IVF or FET cycle.
Fresh Transfer:
In a fresh transfer cycle, day one is marked by the start of stimulation medications, usually on day two to four of a woman’s natural menstrual cycle.
The exact day of transfer is then determined by the timing of egg retrieval and the developmental stage of the embryo. Both of these can vary. For example, ultrasound and bloodwork monitoring may show that more or fewer days of stimulation are needed, shifting the retrieval date forward or backward.
Most cleavage-stage transfers occur three days after retrieval, and most blastocyst-stage transfers occur five days after. However, embryos develop at different rates, and it is not unusual for a blastocyst transfer to take place seven days after retrieval.
Below is a sample calendar for a fresh embryo transfer.
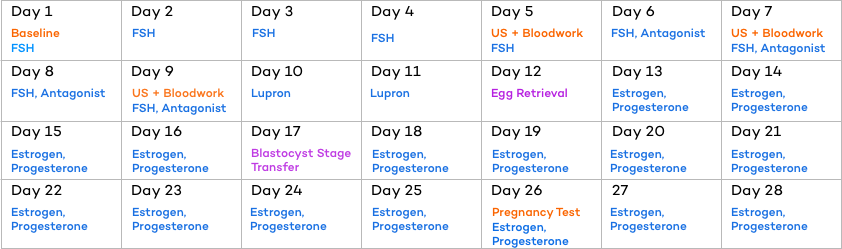
Frozen Transfer:
Like a fresh transfer, every frozen embryo transfer (FET) is tailored to the intended parents’ cycle, based on uterine lining development and the body’s response to medications, if used.
The length of time spent on estrogen before introducing progesterone varies from person to person and is closely guided by ultrasound and bloodwork monitoring. Ultimately, the timing of the transfer is determined by the start of progesterone.
- Cleavage-stage embryos are transferred four days after progesterone begins.
- Blastocyst-stage embryos are transferred six days after progesterone begins.
Below is a sample FET calendar.

What to Expect During Embryo Transfer
Embryo transfers are performed under sterile conditions, usually in a designated transfer room at the fertility clinic.
You will be accompanied by your doctor, a nurse, the embryologist, and often your partner. Anesthesia is not typically required, but a mild relaxant such as Valium may be used to calm nerves and relax the uterine muscles.
Any prescribed medications should be taken exactly as directed, though you may be asked to avoid inserting anything vaginally (such as a suppository) on the morning of the transfer.
Before the procedure, the doctor and embryologist will confirm your name and date of birth against the information on the embryos. The embryologist then loads the embryo into the transfer catheter. At the same time, a speculum is placed in the vagina to allow visualization of the cervix, which is then cleaned.
Using ultrasound guidance, the catheter is gently passed through the cervix and into the uterus, where the embryo is deposited.
The procedure is often compared to a Pap smear. It should not be painful, though you may feel mild discomfort when the speculum is inserted or as the catheter passes through the cervix.
Afterward, you will rest for about 15 minutes before receiving follow-up instructions. Bloodwork is typically scheduled 4 to 7 days after transfer, with a pregnancy test about 10 days later.
What to do Before Embryo Transfer to Improve Chances of Success
There are many steps you can take before an embryo transfer to help improve the chances of success.
Most of these lifestyle and health changes are most effective when started 30 to 90 days before the stimulation phase of IVF, since eggs begin their final stage of development about three months before ovulation.
Supporting this process can enhance egg quality, which contributes half of the embryo’s genetics, and give your treatment cycle the strongest possible foundation.
Diet & Supplementation:
- High-Fat / Low Carb Diet: Eating a high-fat / low carb diet reduces inflammation throughout the body, G.I. tract, and reproductive system. It also aids hormone function since many female hormones are made from cholesterol, which comes from fat.
- OTC Supplements: Various fertility supplements such as co-q10/ubiquinol, inositol, Vitamin D, and many others can be tremendously helpful for women and men. Companies like Molecular Fertility have combined the dozens of recommended ingredients into a few simple products. We generally recommend females take Peak Prenatal, VivoMega Fish Oil, and Ovarian Bloom. For males, we recommend the Male Preconception+ as well as VivoMega Fish Oil.
Prescription Medications:
Various immunological medications can help improve transfer outcomes, particularly after a history of failed implantation. Some immunological medications include:
- Intralipids
- low-dose naltrexone
- HGH
- Antibiotics
- Tacrolimus (Prograf)
- Prednisone
- Aspirin (over the counter)
- Lovenox
- hCG
- IVIG
- Filgrastim (Neupogen)
- Viagra
- Antihistamines (over the counter)
- Metformin
- Orilissa
Surgical Treatment & Immune Therapies:
- Lymphocyte Immunization Therapy (LIT): LIT is a procedure whereby white blood cells from the father to be are isolated from the father’s blood and injected into the skin of the prospective mother to introduce the husband’s immune cells to the woman’s immune system in preparation for pregnancy. LIT therapy is often recommended after many failed IVF cycles and suspected immunologic reasons for failed implantation.
- Platelet Rich Plasma (PRP) Therapy: PRP, a concentrated platelet-rich blood product, helps to stimulate healing and tissue growth and can be used for both ovarian/egg support as well as to improve endometrial thickness and receptivity.
- Endometrial Biopsy: An endometrial biopsy (aka scratch procedure) may be performed before the menstrual cycle of the month you wish to proceed with the transfer can be very helpful. “Scratching” the endometrium lining causes chemicals called cytokines, which promote healing, to be released. This healing process may help encourage better lining development in the following months.
- Intra-uterine hCG: Placing a small amount of Human Chorionic Gonadotropin (hCG) into the uterus prior to transfer is believed to improves the odds of implantation by up to 30%. CNY Fertility encourages the use of 500 IU of intrauterine hCG as part of our embryo transfer protocol to help jump-start the implantation process.
- Endometrial Receptivity Analysis (ERA): An ERA is a test done to evaluate a woman’s endometrial receptivity, or how likely an embryo is to stick. The test is performed to help prevent implantation failure by identifying a woman’s unique and optimum window of implantation.
- Laparoscopy: A laparoscopy is a minimally invasive surgical procedure to visualize the inside of the abdominal and pelvic cavity to diagnose and correct Endometriosis, Uterine Fibroids, Abnormal Growths, and adhesions.
- Hysteroscopy: A hysteroscopy is a minimally invasive diagnostic and corrective procedure done to visualize the inside of the uterus to investigate and correct (if discovered) the source of abnormal uterine bleeding or suspected cause of infertility and miscarriage.
Holistic Therapies:
- Acupuncture: Research has revealed that acupuncture can improve pregnancy rates by up to 65% in women doing in-vitro fertilization treatments .
- Massage: Massage techniques explicitly developed to treat infertility, like the Maya Abdominal Massage, can be used to improve fertility by increasing blood flow to the reproductive organs, relieving blockages, and decreasing inflammation. It can also help to realign the uterus and relieve stress and anxiety often associated with infertility.
- Yoga: Yoga can be used as a supplementary fertility treatment by reducing stress, improving blood flow to the reproductive organs, and balancing the immune system.
What to do After Embryo Transfer to Improve Chances of Success
Most of the preparation for a successful embryo transfer happens well before the procedure.
Once the transfer takes place, there is little that can be done to influence the outcome. However, one supportive measure often recommended is acupuncture immediately after transfer.
Several studies have shown benefits when acupuncture is performed both before and after embryo transfer during an IVF cycle. In fact, fourteen studies published in Fertility and Sterility reported that this approach increased pregnancy rates by 35 to 50 percent. .
After Embryo Transfer Precautions
Implantation of the embryo can occur up to 72 hours after embryo transfer. Post-transfer instructions vary from clinic to clinic. While standard protocol used to be to recommend bed rest, this is no longer the case.
The experts at CNY suggest patients resume their normal routines, but are restricted from strenuous exercise, sex, or taking baths.
We recommend going home, relaxing, and getting a good night’s sleep. Maintain a positive outlook, find ways to relax and connect with your partner during the dreaded “two-week wait” between transfer and pregnancy test. Try not to get too caught up in do/don’t lists. Focus on yourself and do the things you enjoy.
- Remember that women get pregnant all the time without changing their activities.
- Continue to take all medications as instructed.
- Behave as if you’re pregnant: Eat and act just like you’re pregnant.
- Stay active: You can pretty much resume your normal routine. Just avoid strenuous exercise.
- No Sex. Mother Nature must run her course.
- Avoid Extreme Temperatures: This means no hot baths, hot yoga, saunas, heating pads, or electric blankets. They can all raise the temperature of your uterus and should be avoided.
Embryo Transfer Costs:
Fresh Embryo Transfer Cost
The cost of a fresh embryo transfer is typically included in the base price of an IVF cycle, which averages $15,000 to $25,000 nationwide, and $5,800 at CNY Fertility, including standard medications.
Because it is bundled with the overall IVF package, it is difficult to separate out the exact cost of the transfer alone from the other services that are part of the cycle.
Frozen Embryo Transfer Cost
The average cost of a Frozen Embryo Transfer is around $4,000, but ranges from $1,400 (including the procedure and monitoring) here at CNY Fertility to over $6,000 at other clinics around the country.
Which Is More Expensive: Fresh or Frozen?
At first, it may seem like a simple question, but the answer depends on perspective.
A frozen embryo transfer can be viewed as an additional expense, especially if it is used as the first transfer without attempting a fresh transfer.
However, many IVF cycles produce more embryos than can be transferred at once. These extra embryos are frozen for future use, either after a failed transfer or following a successful birth.
In this context, the cost of a frozen embryo transfer is significantly lower than starting a new IVF cycle.
IVF & Embryo Transfer Payment Calculator
Automatically Included
-
{{ tick.item }}
Sample Payment Calculator: Self Pay Pricing
-
{{getTreatmentName()}} {{ treatment_price_discount|toCurrency }}
National Average {{ this.treatment_price_others|toCurrency}} -
{{ treatment.data.price.monitor.remote.label }} Remote Cycle Management {{ total_monitor.cny | toCurrency }}{{ treatment.data.price.monitor.in_house.label }} In House Monitoring {{ total_monitor.cny | toCurrency }}{{ treatment.data.price.monitor.remote.note_calc | stripHTML }} {{ treatment.data.price.monitor.in_house.note_calc | stripHTML }} Third-party fixed fee (SAMA) Third Party {{ total_monitor.others | toCurrency }}{{ treatment.data.price.reciprocal_ivf.note_calc || "Reciprocal IVF requires both partners to be monitored" }} {{ treatment.data.price.frozen_transfer.note_calc_monitor || "" }}
-
-
{{ treatment.data.price.frozen_transfer.label }} Frozen Transfer {{treatment.data.price.frozen_transfer.cny|toCurrency}}
-
{{ treatment.data.price.cryo_preserve.label }} Cryopreservation + 1yr Storage {{treatment.data.price.cryo_preserve.cny|toCurrency}}{{treatment.data.price.cryo_preserve.note_calc | stripHTML}} Third Party {{treatment.data.price.cryo_preserve.others|toCurrency}}
-
{{ treatment.data.price.genetic_testing.label }} Genetic Testing {{treatment.data.price.genetic_testing.cny|toCurrency}}{{treatment.data.price.genetic_testing.note_calc | stripHTML}} Third Party {{treatment.data.price.genetic_testing.third_party|toCurrency}}
-
{{ treatment.data.price.medication.label }} Medication Estimate {{total_medication.cny|toCurrency}}{{total_medication.note_calc | stripHTML}} Third Party {{total_medication.third_party|toCurrency}}
-
{{ treatment.data.price.medication.label }} Medication Estimate {{total_medication.cny|toCurrency}}{{total_medication.note_calc | stripHTML}} Third Party {{total_medication.third_party|toCurrency}}
-
{{ treatment.data.price.zymot.label }} ZyMōt Sperm Processing ${{treatment.data.price.zymot.cny}}{{ treatment.data.price.zymot.note_calc | stripHTML}} Third Party ${{treatment.data.price.zymot.third_party}}
-
{{ treatment.data.price.pregmune.label }} Pregmune Reproductive Immunology Testing {{treatment.data.price.pregmune.cny|toCurrency}}{{ treatment.data.price.pregmune.note_calc | stripHTML}} Third Party {{treatment.data.price.pregmune.third_party|toCurrency}}
-
{{ treatment.data.price.donor_eggs.label }} Donor eggs {{total_donor_eggs.cny|toCurrency}}{{treatment.data.price.donor_eggs.note_calc | stripHTML}} Third Party {{total_donor_eggs.others|toCurrency}}
-
{{ treatment.data.price.donor_sperm.label }} Donor sperm {{treatment.data.price.donor_sperm.cny|toCurrency}}{{treatment.data.price.donor_sperm.note_calc | stripHTML}} Third Party {{treatment.data.price.donor_sperm.others|toCurrency}}
-
{{ treatment.data.price.donor_eggs.label }} Donor Package {{total_donor_package.cny|toCurrency}}{{treatment.data.price.donor_package.note_calc | stripHTML}} Third Party {{total_donor_package.others|toCurrency}}
-
{{ treatment.data.price.gestational_surrogacy.label }} Gestational Surrogacy {{treatment.data.price.gestational_surrogacy.cny|toCurrency}}{{treatment.data.price.gestational_surrogacy.note_calc | stripHTML}} Third Party {{treatment.data.price.gestational_surrogacy.others|toCurrency}}
-
{{treatment.data.price.split_cycle.label ? treatment.data.price.split_cycle.label : "Split Cycle Discount" }} {{discount_split_cycle|toCurrency}}
-
5% Military & Veteran Discount {{discount|toCurrency}}
-
Installments Fee {{finance.fee|toCurrency}}
-
Total to CNY {{total.total | toCurrency}}
Estimated 3rd Party Costs {{total.third_party| toCurrency}}
Grand Total {{(total.total + total.third_party)| toCurrency}}
National Average: {{total.national|toCurrency}} -
Down Payment to CNY{{finance.payment_down_amount|toCurrency(2)}}
-
Monthly Payment to CNY{{finance.monthly_payment|toCurrency(2)}}
{{ treatments[treatment_selected]['data']['footnote'] }}
The above calculation is for simulation purposes only. It is reflective of self-pay pricing, includes highly variable estimates paid to CNY and third parties, and national averages obtained through internal research, FertilityIQ, ASRM, and Resolve. Billing through insurance will likely result in substantially different fees. CNY Fertility does not warrant or guarantee any price for services conducted or rendered by a third party and recommends everyone obtain written estimates from any medical facility involved in your treatment as well as verification of coverage from your insurance company prior to beginning treatment.
1 USD = {{currency.rates[currentCurrency]}} {{currentCurrency}}
Last Update {{currency.last_update}}
To learn more about the cost of IVF and Embryo Transfers, head here.
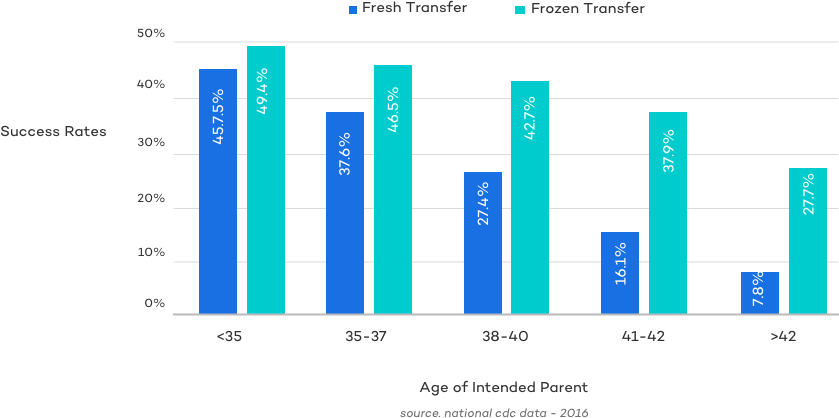
Fresh vs. Frozen Success Rates:
As you can see below, the overall success rates of frozen embryo transfers is higher when looking at large scale data from the CDC.
Despite the success rates outlined above, and systematic reviews suggesting that frozen embryo transfers may have higher success rates than fresh transfers, the question of which approach is best remains one of the most debated topics in fertility medicine.
The widespread adoption of frozen transfers has been fueled by advances in embryo freezing techniques, which have made FETs highly effective. Yet the ongoing debate highlights that there is no one-size-fits-all answer and that the choice between fresh and frozen transfer must be made on an individual basis.
With that in mind, let’s review the two biggest factors that influence the success of an embryo transfer:
- Embryo Quality: A healthy embryo without genetic defects is more likely to implant and result in a healthy baby.
- Uterine Quality & Receptivity: Uterine receptivity plays a large role in embryo implantation. If the uterus isn’t ready to receive the embryo, it’s hard for the embryo to stick. Timing and lining are critical.
Embryo Quality
Before the development of vitrification, embryos were frozen using a much slower process that often damaged them. Survival rates after thawing were low, and even when embryos did survive, their quality was frequently compromised.
With vitrification, however, embryos can now be frozen and thawed with minimal damage. This advancement allows frozen embryos to maintain their quality, making outcomes from frozen transfers nearly identical to those of fresh transfers.
Uterine Receptivity
As noted earlier, the gonadotropin medications used in IVF to stimulate the ovaries can place additional biological stress on the body. In some cases, this makes it more challenging for the uterus to be optimally prepared to receive an embryo.
That said, fresh transfers can still achieve success rates comparable to frozen transfers. Each case should be evaluated individually, with close attention to uterine lining development and hormone levels, to ensure the endometrium is receptive at the time of transfer.
A Patient-Centered Approach
Other studies have shown a more nuanced approach that considers the importance of specific hormone levels in determining uterine receptivity and thus when to transfer fresh embryos and when to pursue a freeze-all followed by a frozen transfer cycle.
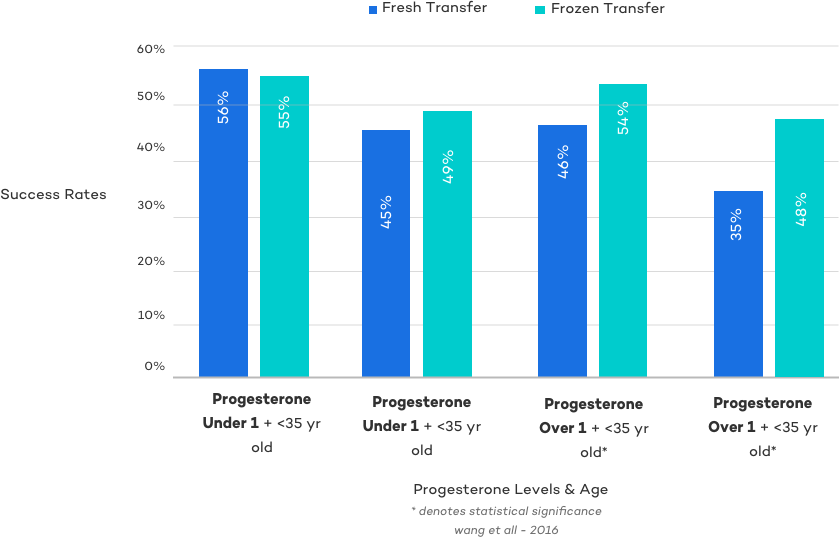
As this study showed, fresh transfers can sometimes achieve success rates comparable to frozen transfers. Since cost is a significant factor for many patients, fresh transfers may be the preferred option in certain cases. For this reason, a patient-centered approach is more appropriate than rigid, one-size-fits-all guidelines.
Today, most clinicians and practices consider estrogen and progesterone levels, the thickness of the endometrial lining at the time of trigger, and the patient’s own preferences when deciding whether to proceed with a fresh or frozen transfer.
Embryo Transfer Risks
Even though the embryo transfer process is brief, there is some inherent risk, including:
- cramping (fairly common)
- vaginal bleeding (mild bleeding fairly common)
- perforation of the uterus (extremely rare)
- infection (rare)
Also, given the success rates of each embryo transfer top off around 50%, there is a fairly high risk that the embryo fails to implant and no pregnancy occurs. There is also the risk of a multiple gestation, which carries a chance for a significant number of medical complications for both the mother and fetuses. The risk of multiples is exponentially higher when transferring more than one embryo.
Embryo Transfer: The Bottom Line
An embryo transfer is the final step in the IVF process, when an embryo is carefully placed into the uterus in the hope it will implant and develop into a healthy pregnancy.
There are several types of transfers, and the timing can vary widely from patient to patient. Ultimately, your fertility doctor, embryologist, and care team will guide you through each decision to give you the best chance of success in your individual case.
Article Sources

For IVF Grant Announcements, Fertility News and More!