Getting Pregnant 101

Getting pregnant – Birds do it. Bees do it. Even educated fleas do it. Well, not all in the same way and certainly not like humans, but Cole Porter got it right. Reproduction is a natural component of all life. It sounds pretty easy. And it looks pretty easy too, judging by the number of pregnant women walking around. But is it really? When you’re actively trying to conceive or experiencing recurrent pregnancy loss, it certainly doesn’t seem so.
Why? Because it’s not. Reproduction requires an astronomically large number of partially random biological events to be perfectly aligned. Let’s start with some fast facts before we really break down what it takes to get pregnant.
Fast Facts about Getting Pregnant
- Successfully conception requires a healthy egg, healthy sperm, open fallopian tubes, a uterus that can sustain a pregnancy, properly timed intercourse, a healthy mother, and hormones to support each event in the conception process and pregnancy.
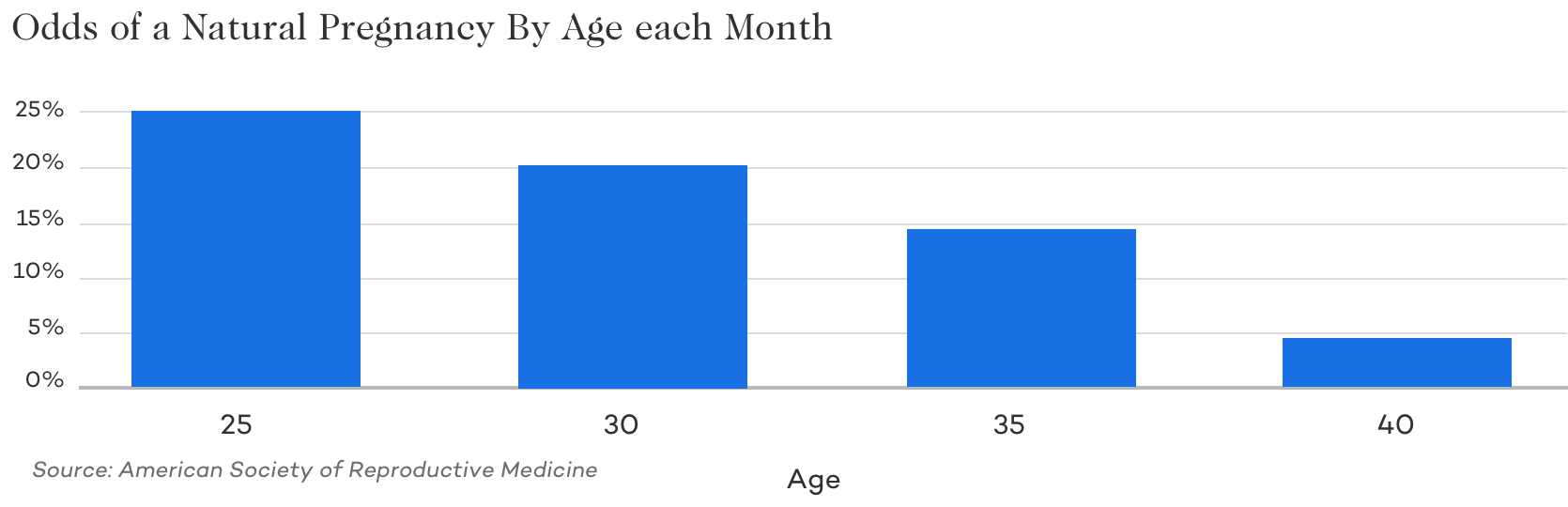
- Even young fertile couples only have a 20-25% chance of conceiving each month.
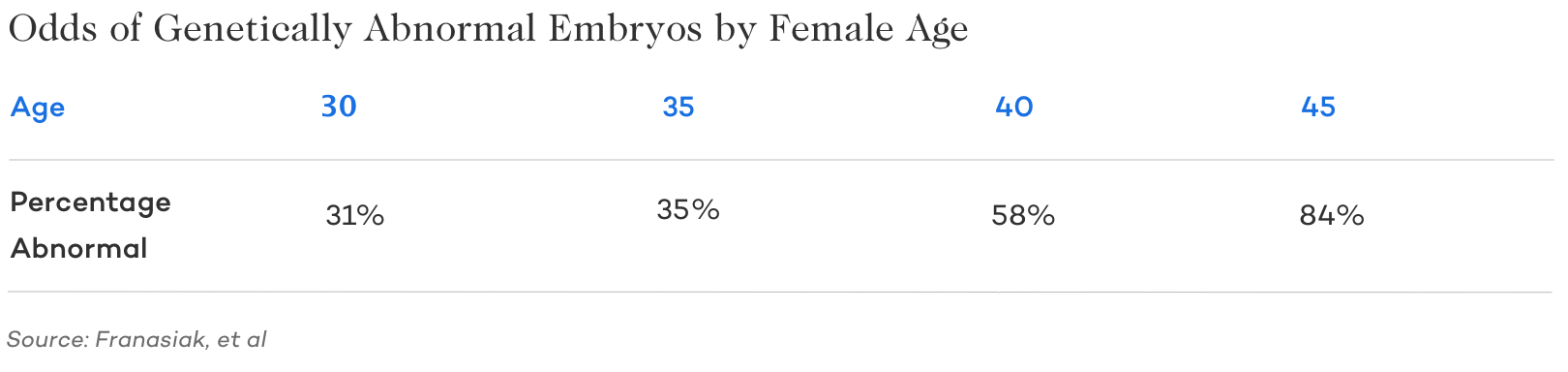
- The likelihood of abnormal eggs increases as a woman ages, making conception more challenging and miscarriage more likely.
- There are a number of fertility treatments that can be used to overcome both male and female causes of infertility. Unless contraindicated, most couples start with the least advanced/invasive treatments (like ovulation induction or Intrauterine Insemination IUI) when trying to conceive naturally fails and only progress to more involved treatments, such as In Vitro Fertilization (IVF), if they are not successful.

Basics of What’s Needed to Get Pregnant Naturally
Even though it seems like some couples get pregnant just by thinking about it, conception is a whole lot more complicated than that, miraculous even.
In order for a healthy pregnancy to occur, there are a few critical elements that are absolutely essential for getting pregnant:
- Healthy egg and ovulation
- Healthy sperm in the ejaculate
- properly timed intercourse
- healthy open tubes
- healthy uterus
- healthy mother
But that’s just a quick overview, let’s dig in for those who really want to know what it takes to get pregnant.
A Healthy Egg and Ovulation
In order to conceive, it takes a healthy egg and that egg being released from the ovary. Women are born with all of the eggs they will ever have. A woman’s number of potential eggs is actually at its peak before she’s even born. At birth, the average female has around 2 million potential eggs. How many of these future eggs are ‘healthy’? Unfortunately, not all of them. Even women in their 20s have a number of genetically abnormal eggs in the mix. There’s no way to test egg quality besides actually fertilizing the egg. There’s no bloodwork or special test that will tell us if you have genetically normal eggs. What we do know is that the older you are, the more genetically abnormal eggs you produce. The ability to get pregnant is directly connected to egg quality. If the ovulated egg is not genetically normal, it will likely fail to fertilize, fail to implant, or result in a miscarriage.
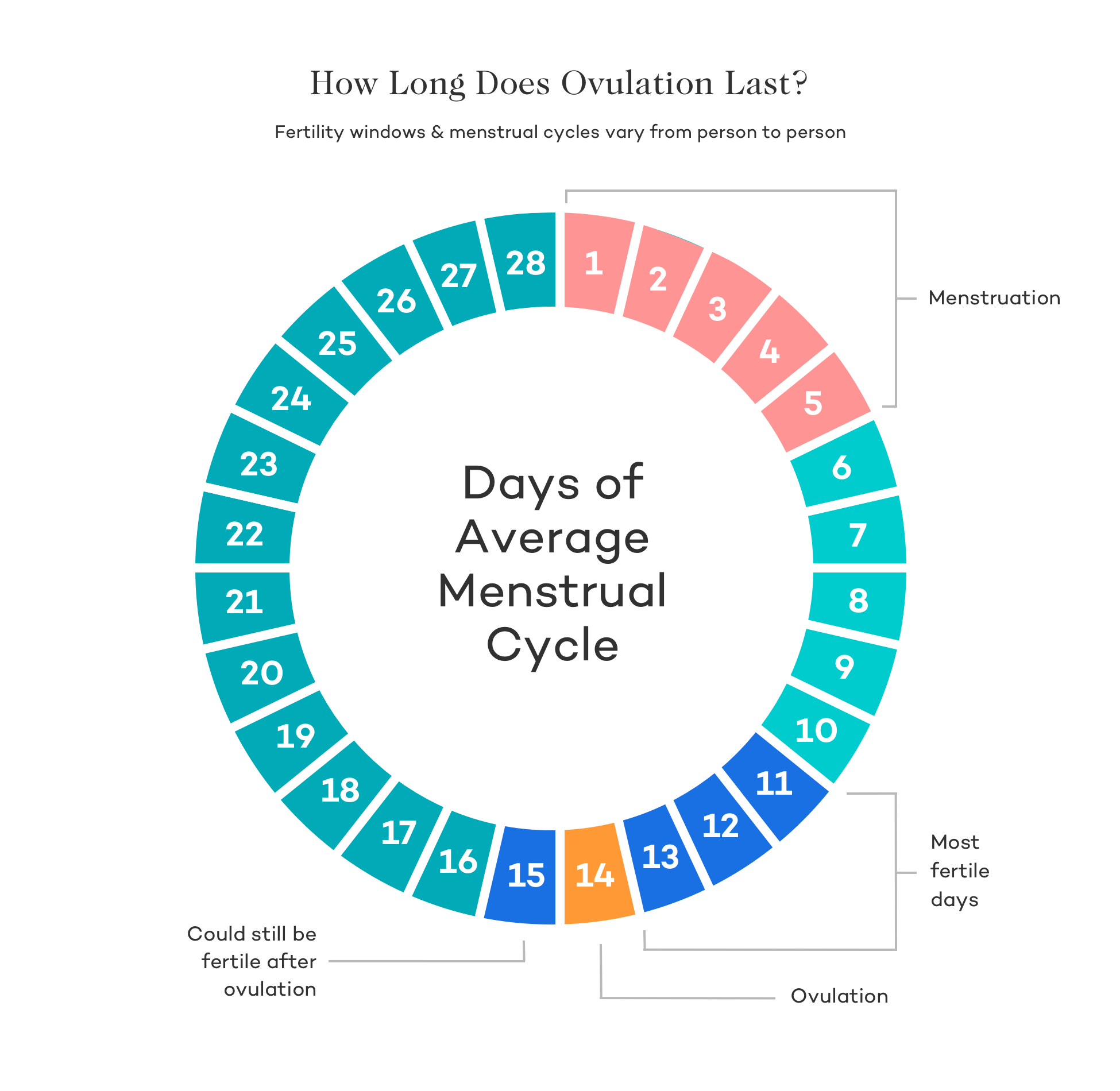
In order for the egg to be available for fertilization, it must be released from the ovary in a process known as ovulation. Follicles are structures on the surface of the ovary that contain microscopic, immature eggs. Hormones released by the endocrine system help follicles develop. Each month, the largest follicle releases a mature egg that gets pulled into the distal portion of the fallopian tube where it waits to be fertilized. Ovulation typically occurs around day 14 of a 28-day menstrual cycle; however, not everyone has a cycle that’s 28-days long. It can range from 21-days up to 35 or 36 days, so the exact timing of ovulation can vary from woman to woman. Ovulation is the most fertile time during your menstrual cycle.
Some women don’t ovulate regularly because of PCOS or other medical conditions. This can be a problem for conception. But there are various medications that can be used to make the body ovulate.
Healthy Sperm in Ejaculate:
While women generally produce a single egg each month, men can release around 100 million sperm each time they ejaculate. Not all of these sperm are healthy, and not all of them will make the journey through the vagina, cervix, and uterus and into the fallopian tube. But all it takes is one sperm to swim its way to the egg. Experts believe this process may be nature’s way of allowing only the healthiest sperm to fertilize the egg, which in turn provides the best chances of having a healthy baby. What makes for healthy sperm? Good sperm count, motility, morphology, and volume. A high concentration of sperm cells in a semen sample is a marker for good sperm quality. Morphology refers to the shape of the sperm, or what the shape of the sperm head and the size of the sperm looks like under a microscope. Healthy sperm have rounded heads and long, strong tails. The head shape is important as it affects the sperm’s ability to dissolve the outer surface of an egg and fertilize it. Motility refers to the sperm’s ability to move, which is critical to reaching the egg. A minimum volume of semen is necessary to carry sperm cells through the female reproductive tract. All of these characteristics play a role in sperms’ ability to get to and penetrate an egg.
Learn more about improving sperm!
Properly Timed Intercourse
As the old saying goes, “Timing is everything.” It stands true for jokes, finding jobs, and conception. For pregnancy to occur, sperm must be present just before or at the time the egg is released. Healthy sperm can live for up to 5 days in a woman’s body, but an egg survives for just 12-24 hours after ovulation. If it doesn’t get fertilized, it disintegrates into the uterine lining and is shed during the woman’s monthly period. For the best chances of conception, fertility doctors recommend having intercourse 4-5 and again 2-3 days leading up to ovulation. Ideally, you want to have sperm ready and waiting in the fallopian tubes, so that they can do their thing as soon as the egg is released. Or, if you don’t want to worry too much about timing, get frisky 2 times a week every week.
Remember, it’s not far to us, but for microscopic sperm – that’s a long way to swim, so it takes a few days to get into the fallopian tubes.
Healthy, Patent Tubes: A Place for Sperm + Egg to Meet
The fallopian tubes perform critical functions in reproduction, such as picking up the egg from the ovary, transporting the egg, fertilization, and embryo transport from the fallopian tube to the uterus.
Think of your fallopian tubes as a fertility superhighway. For sperm, egg, and the eventual embryo to travel where they need to go, you want open roads with no lane closures. This means healthy fallopian tubes with no scarring, adhesions, damage, or blockages. “Patent” means open, but open tubes don’t necessarily mean functioning. Tubes that are open but have scarring may not be able to perform all the necessary functions. Doctors can confirm tubal patency using a hysterosalpingogram (HSG), a sonohysterosalpingogram (SSG, or Saline Sonogram) or a Laparoscopy.
Healthy Uterus: A Safehaven for Baby to Grow
A healthy uterus is critical to embryo implantation and the continued development of a fetus. The uterus is the first home for a growing baby. Key markers of a healthy uterus include a sufficiently thick (around 7 to 8 mm) and a “receptive” endometrium (the lining of a woman’s uterus), and absent of uterine fibroids, adhesions, scar tissue, and endometriosis which might impair implantation and growth. Good blood flow and strong uterine muscles also help ensure
Women with inactive lifestyles risk reduced blood flow to the uterus that can lead to shrinkage of the endometrial lining. Lack of blood supply to the uterus may also lead to the formation of adhesions and scar tissue. Physical movement is key. Yoga, Tai Chi, stretching, and walking are good activities. In that same vein, strenuous exercise can pull blood flow from your core, which is also not helpful. Regular activity also strengthens and tones the uterine muscles to support the normal functioning of the uterus.
Balanced Hormones
Hormones are crucial to conception and successful implantation and growth of an embryo. They are the catalyst for an order of events that requires precise order and timing. If hormone levels are too high or too low, a disruption in the chain can occur that prevents a necessary process from happening. Men need the right levels of testosterone, FSH, and LH to produce sperm. Women need the right levels of FSH, LH, estrogen, and progesterone at exactly the right time to trigger follicle growth, ovulation, endometrial growth, and other events in the conception cycle. Even tiny problems can have a huge impact and completely disrupt the process resulting in an inability to conceive.
Healthy Mother
Although the word “healthy” means different things to different people, preconception health is an important part of the conception process. Women looking to conceive should:
- Not smoke or use recreational drugs and limit alcohol consumption.
- Discuss any prescription drugs you might be taking with your provider to be sure they are safe
- Avoid working with or using hazardous chemicals at home or in the workplace.
- Use relaxation techniques like yoga, acupuncture, and massage to moderate stress levels.
- Avoid drinking high levels of caffeine as they can contribute to delayed conception
- Incorporate regular movement and low-intensity exercise into your routine
- Track your menstrual cycle
- Get enough sleep
- Eat a healthy full-fat diet with low to no carbs and medium protein. This can reduce inflammation and improve hormone function.
- Consider taking verified fertility supplements such as folic acid, Co-Q10/ubiquinol , inositol , Vitamin D and more.
- Maintain an ideal weight – being overweight or underweight can affect conception.
- Mindset is also important. Practicing meditation and prayer can help manage the stress of life and help build a positive belief system.
And since egg development begins up to 90 days before conception, for optimum effect, it’s important to make these lifestyle changes three-months or more before you begin trying to conceive.
Learn more about boosting female fertility here.
Key Biological Steps of Getting Pregnant Naturally
Conception is a carefully timed process. Everything must happen when and where it’s supposed to in order for pregnancy to occur. Here are the key steps:
Egg and Sperm Develop without Major Genetic Abnormalities:
As mentioned previously, even young fertile women still produce some genetically abnormal eggs. As women age and egg quality naturally declines, the percentage of abnormal eggs also increases . This is why women in their 40s have a difficult time conceiving with their own eggs compared to younger women (unless they froze eggs previously and at a younger age).
Similarly, it’s not uncommon for men to produce a certain number of abnormal sperm. Most men have a large percentage of abnormal sperm morphology, with only 4-15% of their sperm being considered normal. Sperm can be considered normal as long as more than 4% are “morphologically normal.” Because there are so many sperm, those 4% may be all it takes to go the distance.
Abnormal sperm can be caused by many factors, but the most common are drivers are age and genetics. As a man ages, sperm tend to have a higher number of genetic abnormalities. For example, tt’s more likely for a man in his 50s or 60s to have a higher number of abnormal sperm than it is for a man in his 20s.
However, that said, in reality, many men can successfully father children into their 70s and even older in part because it’s a numbers game. Whereas women produce just one egg a month, men are releasing millions of sperm. Even a small percentage of several million is more than enough sperm to successfully fertilize an egg.
The best way for a man to check their sperm is with a semen analysis. If there are signs of male factor infertility there are many treatments that can help (more below) as well as many ways to improve sperm count, motility, and quality.
One of the Ovaries Releases a Mature Egg
In women who ovulate normally each month, hormones that come from the brain called Follicle Stimulating Hormones (FSH) cause a number of immature follicles within the ovary to begin to develop. These follicles produce estrogen, which signals the uterus to begin preparing for pregnancy. Cells in the lining of the uterus (the endometrium) need to grow quickly to create a receptive environment for the embryo. Out of these follicles, there will be one (sometimes two) dominant follicle that gets quite big and releases an egg. The remaining follicles do not mature, die off, and are reabsorbed by the body. Luteinizing Hormone (LH) from the brain triggers ovulation by causing the egg to mature and the follicle to rupture, thereby releasing the egg from the ovary.
The Egg is Picked Up by the Fimbria and Enters the Fallopian Tube
Finger-like projections from the fallopian tube called fimbria are able to move and sweep the just-released egg into the end of the fallopian tube. For fertilization to occur, there needs to be sperm waiting in the fallopian tube for the egg when it’s ovulated or very soon thereafter. Ideally, intercourse occurs 72-hours prior to ovulation, so sperm are already present when the egg enters the fallopian tubes. After the release of the egg, the ruptured follicle is transformed into the corpus luteum, which releases progesterone and estrogen that’s essential for implantation in the uterus a few days later.
Sperm Swim Through the Cervix, Uterus, and Enter the Fallopian Tube
Thousands of sperm make it past the cervix and into the uterus, but only a fraction of those sperm will make it up and to the end portion of the tubes where the egg is waiting. The sperm’s entire journey is just a couple of inches, but for some small cells, it is a Herculean task. Ideally, a sperm count of 20-40 million sperm is needed for there to be enough sperm to survive the journey and meet the egg. As sperm move through the vagina to the cervix and beyond, there is a constant attrition to the number of sperm that survive and continue on. Millions become thousands and then just hundreds.
Sperm and Egg Meet and Fertilize
Lots of sperm “attack” the egg and try to pierce its outer layer until one of them succeeds, and fertilization occurs.
Fertilized Egg (Embryo) Travels Back Down Tube into Uterus
Once the egg is fertilized, development continues within the fallopian tube as it travels towards the uterus. Cells of the egg divide and begin to create the cells that will become the embryo and placenta. Around Day 3, the embryo has about eight cells and is called a cleavage stage embryo. By day 5-8, the embryo is now called a blastocyst, has 150-250 cells, and has moved into the uterus where it will hatch and begin to implant in the lining of the uterus.
Embryo Implants and Thrives in Uterus
Implantation occurs about six days after ovulation. The endometrium sends signals to the embryo pulling it in to implant. The thicker the lining, the “louder” these messages are to the embryo, and the more likely it is to implant successfully. When implantation occurs, the hormone hCG (Human Chorionic Gonadotropin) is released. hCG is the “pregnancy hormone” that at-home pregnancy tests look for. hCG keeps the corpus luteum alive, so it continues to release estrogen and progesterone, supporting the endometrium as it nourishes the development of the embryo until the placenta is formed.
It that all happens correctly you’re officially pregnant until proven otherwise.
A Guide to Getting Pregnant Naturally
Timing Intercourse & The Fertile Window
In order to best calculate when you’re most fertile, it’s helpful to understand the menstrual cycle and what happens when. The first day of your period is considered Day 1 of your cycle. On Days 1 through 14, your body is focused on egg growth and maturation and womb preparation. This is called the Follicular Phase. In a 28-day cycle, most women will ovulate, or release an egg, around Day 14, beginning the Luteal phase of your cycle during which pregnancy can occur.
The fertile window is the days in a woman’s cycle where it is possible to get pregnant. Once the egg is ovulated, it lasts for just 12 to 48 hours before it can no longer be fertilized. But remember, it’s quite a far swim for the sperm to make, so the most fertile days (the days it is best to have intercourse on) actually occur before ovulation. In total, the fertile window is around five days though some studies claim it may even be as long as ten days .
To become pregnant, the best time to have sex is during the 72 hours leading up to ovulation. At this point, sperm are likely to survive (remember that sperm can live for up to 5 days inside your body) and be ready and waiting in the fallopian tubes as soon as the egg is released at ovulation.
Because the egg survives for a maximum of 48 hours after ovulation, timing is critical. It’s important to understand the body’s natural signals for approaching ovulation. Ovulation can be tracked via a few different methods, including:
- changes in vaginal secretions
- body temperature
- ovulation predictor kits
- fertility clinic monitoring
Changes in Vaginal Secretions
The same hormones that control your menstrual cycle also make your cervix produce mucus. This is that sometimes-sticky stuff that comes out of your vagina as discharge. You may find it in your underwear or on toilet paper when you wipe. Mucous production is regulated by the ratio of progesterone and estrogen levels in the blood. Throughout your cycle, it changes in appearance, texture, and elasticity.
Cervical Mucus Timeline:
- Early Cycle (Days 1–5): This is when menstruation/bleeding occurs.
- Post-Period (Days 5–10): At first, there is little or no discharge (the Dry Phase), but sticky, glue-like discharge that can be yellow or white follows during the Sticky Phase.
- Pre-Ovulation (Days 10–14): The body starts to produce more estrogen. Discharge thins and looks cloudy and lotion-like during the Creamy Phase. You may notice in on your underwear. A few days before ovulation, your cervical mucus becomes clear and slippery, like the consistency of egg whites. This is the type of cervical mucus that allows sperm to move past the cervix and up into the uterus. This is the beginning of the Sticky Phase.
- Ovulation (Day 14): On the day of ovulation, cervical fluid is very wet and viscous. You may be able to stretch the fluid an inch or more between your fingers.
- Post-Ovulation (Days 14–22): After ovulation, the body releases progesterone, which dries up cervical fluid. Discharge may look cloudy again and become thicker.
- Pre-Period (Days 22–28): As your period approaches, the discharge becomes a glue-like consistency once again. There tends to be little or no discharge 1–2 days before menstruation.
Detecting Ovulation by Change in Basal Body Temperature:
Basal Body Temperature (BBT) is your body’s temperature when you’re at complete rest. It changes based on a number of factors, including your hormones. When you ovulate, progesterone causes your temperature to rise slightly and remain higher for about two weeks until just before your period starts, when progesterone levels drop. When this happens, it causes your basal body temperature to drop too, unless you’re pregnant. If you conceive, your temperatures will remain higher because progesterone levels remain high.
Tracking your BBT is a way to determine when you’ll ovulate every month. To be accurate, you must take your temperature every morning at the same time before you get out of bed or move around. Don’t go to the bathroom or pick up laundry before you take your temperature. This could cause it to rise slightly, but enough to make your chart inaccurate. Take your temperature before you even pull down the covers!
You’ll need:
- A thermometer that’s accurate to 1/10th of a degree (e.g. 98.6° 98.7°)
- A BBT chart or notebook to record dates/temperature or an app or computer program that helps you keep track and note trends
Starting on the first day of your period, take your temperature every morning at the same time (+/- 30 minutes is okay). Setting an alarm for the same time every day is an easy way to stay consistent. Note your waking temperature and the time. Your temperature may rise or fall slightly each day. When you see three higher-than temperatures in a row, ovulation most likely occurred on the day before the first higher temperature.
After several months of charting, you should begin to recognize some patterns and be better able to predict ovulation day. Some (but not all) women experience a dip in temperature the day they ovulate, and then they experience their first rise in temperature the next day. Be sure to note when you ovulated each month. Tracking your cervical mucus in combination with taking your BBT can also be helpful in confirming ovulation.
Use your charts to predict trends and identify your fertile window. If you kept a chart for three months and ovulated on Days 12, 14, and 15, respectively, you know that your fertile window for the next month should occur between Days 9-16. For the best chances of conception, plan to have sex during these days. Many couples plan to have sex every other day during the week before ovulation.
Ovulation Predictor Kits:
Another tool women can use to help them determine the best days to conceive is an at-home ovulation predictor kit (OPK). OPKs test for luteinizing hormone (LH) in your urine. LH levels spike just before ovulation. This is called the LH surge. It happens about 36 hours before ovulation. The kits come with several test strips. Sometimes they resemble home pregnancy tests, and they are used in much the same way. You pee in a cup or pee on the test strip. When the second line is as dark or darker than the first line, your LH levels have surged, and it’s time to start having intercourse for the next two or three days. Every test kit has slightly different testing instructions, so be sure to fully read the enclosed information carefully, so you understand how to use the kit and interpret results.
Follicular Monitoring:
While checking your cervical mucus, BBT, and using an at-home OPK are things you can do at home to track your most fertile days, a fertility center can also predict ovulation by monitoring follicles and hormone levels. With any kind of fertility treatment, monitoring follicles and hormone levels via blood tests are used to optimally schedule trigger shots, IUIs, or egg retrievals. Ovarian follicles are monitored on ultrasound as they grow and mature. A dominant follicle will grow around 2-3 mm per day and must be checked every couple of days. Your doctor can tell by the size of your follicle(s) and the thickness of your uterine lining how soon you will ovulate. At least one follicle will reach between 17-27 mm just before ovulation.
Monitoring appointments usually begin on Day 2, 3, or 4 or your menstrual cycle. Your first appointment will be a baseline appointment to establish starting levels of certain hormones, number and size of follicles, and your uterine lining thickness. For patients with natural (non-mediated) cycles, 2 to 3 follicular scans during a cycle are all that may be needed.
Does Position Matter when you’re trying to get pregnant?
Is “missionary” best? It seems to be a commonly held belief, but the research on this topic is somewhat limited and mainly comes from IUI studies. Any position that delivers sperm near the cervix can lead to pregnancy. Some positions allow the man to penetrate deeper and closer to the cervix (i.e., rear entry), which may be helpful, but there aren’t studies to support this. Also, if the man ejaculates while the woman is on her back, that may improve conception odds based on an IUI study that looked at women who laid flat for 15 minutes after insemination and compared them to women who immediately got up. Conception rates were higher for the women who stayed flat on their backs.
There’s no wrong way to do it when you’re trying to get pregnant. In fact, sexual arousal for both the man and woman may trump position. Studies have shown the longer foreplay and higher arousal in men can increase sperm count. And women who achieve orgasm may boost their conception rates according to this study .
While hot sex or inventive position won’t cure infertility, they can keep partners feeling emotionally connected, add renewed excitement, and keep things fun with the pressure of “trying” each month starts to feel routine.
Does Lubrication Help or Hurt Your Chances of Getting Pregnant?
Unless you absolutely must use a lubricant, most reproductive endocrinologists would recommend you do without. Vaginal lubricants have been found to damage sperm and interfere with their ability to travel to the uterus to fertilize an egg. Instead, they recommend that your focus on additional foreplay to boost your own natural lubrication. Most women report needing at least 15-20 minutes of kissing, hugging, and touching to get in the mood.
Most lubricants aren’t sperm-friendly. Between its higher acidity and thickness, a lubricant can impede sperm’s ability to travel. Cervical mucus is the perfect acidity for sperm, while lubricants tend to be acidic enough to kill sperm.
Some couples find warm water works well enough as a lubricant. Water isn’t toxic to sperm and won’t interfere with the sperm’s ability to reach the cervix.
If lubricant becomes a necessity, choose one that’s been shown in clinical trials to be safe and effective for conception. They are usually clearly marked as “fertility-friendly” lubricants.
Odds of Getting Pregnant by Age
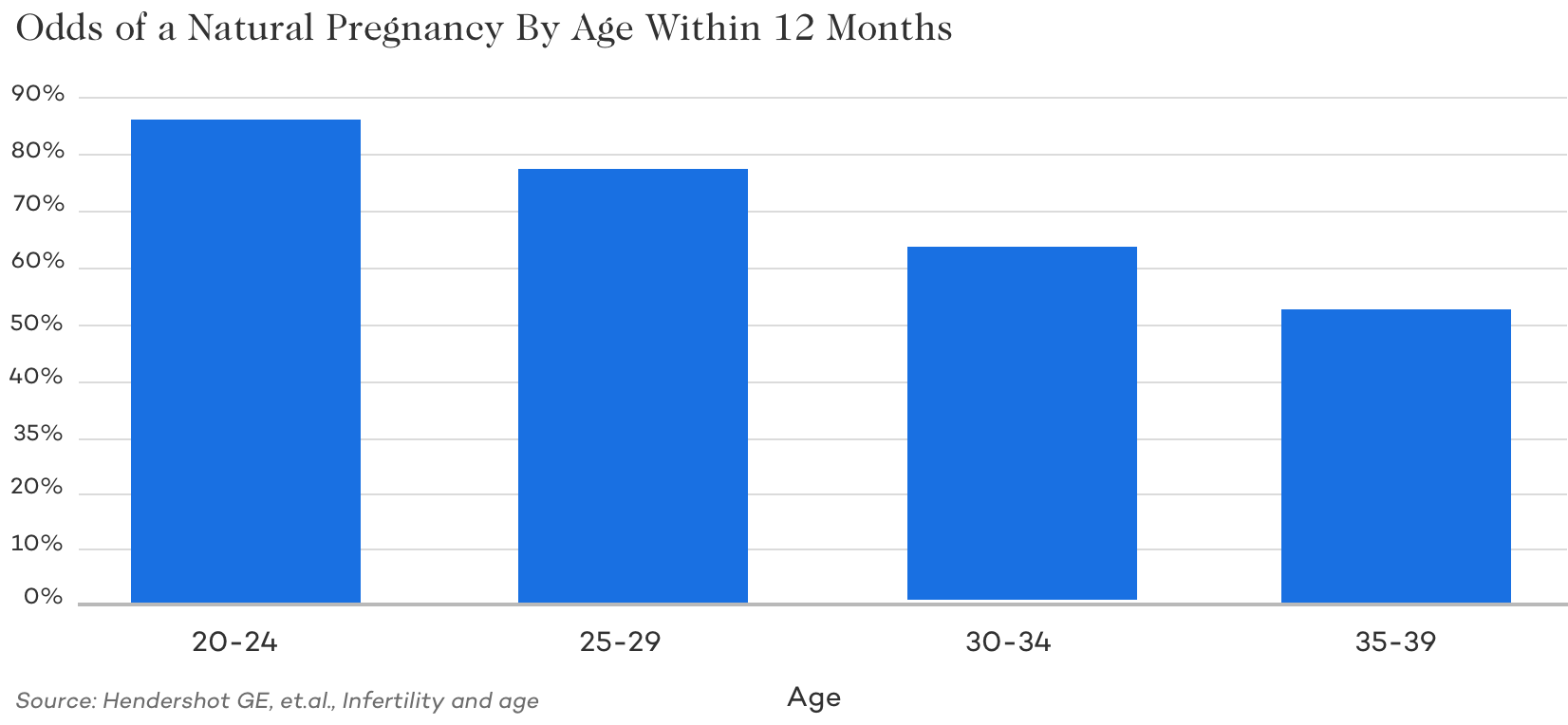
Now that you’ve read about everything that has to happen with perfect precision, it’s easy to understand why getting pregnant isn’t a slam dunk for woman at any age. Even the youngest, healthiest, most fertile women among us still only have a 25% chance of getting pregnant each month because of the narrow fertilization window and egg abnormalities that naturally occur at any age . Why does it eventually happen? Repetition.
Even though a woman has a small chance of getting pregnant each month, her odds of conceiving over six months or a year are much higher. A woman in her early twenties has over an 80% chance of conceiving if she and her partner try to conceive every month over the course of a year. Unfortunately, just like the odds per month drop with age, so do the odds of getting pregnant within a year. Of course, this data may not be at all close to your specific circumstances and could be significantly higher or lower. When in doubt, it’s best to seek help from a fertility specialist.
For example, those with PCOS who are not ovulating regularly or at all would have a lot lower odds of getting pregnant. Similarly, those with little to know sperm would have much lower odds. On the opposite side of the spectrum, those with no fertility issues would likely have higher odds.
Why the Odds of Getting Pregnant Decline Over Time:
Egg Quality:
Like our skin and our bodies, our eggs age right along with the rest of us. As eggs age, they are more likely to become chromosomally abnormal. This means there are small errors in the DNA. Abnormal DNA can lead to cells not functioning correctly, and in the case of an egg, it may not allow for successful fertilization or optimal fetal health development if fertilization does occur. In a woman’s early 20s, 90% of eggs are genetically normal. By her mid-40s, less than 20% of a woman’s eggs remain healthy.
Not only does egg quality decline, but egg quantity does as well. As women approach menopause, their number of remaining eggs begins to decline making conception less and less likely.
Egg Count:
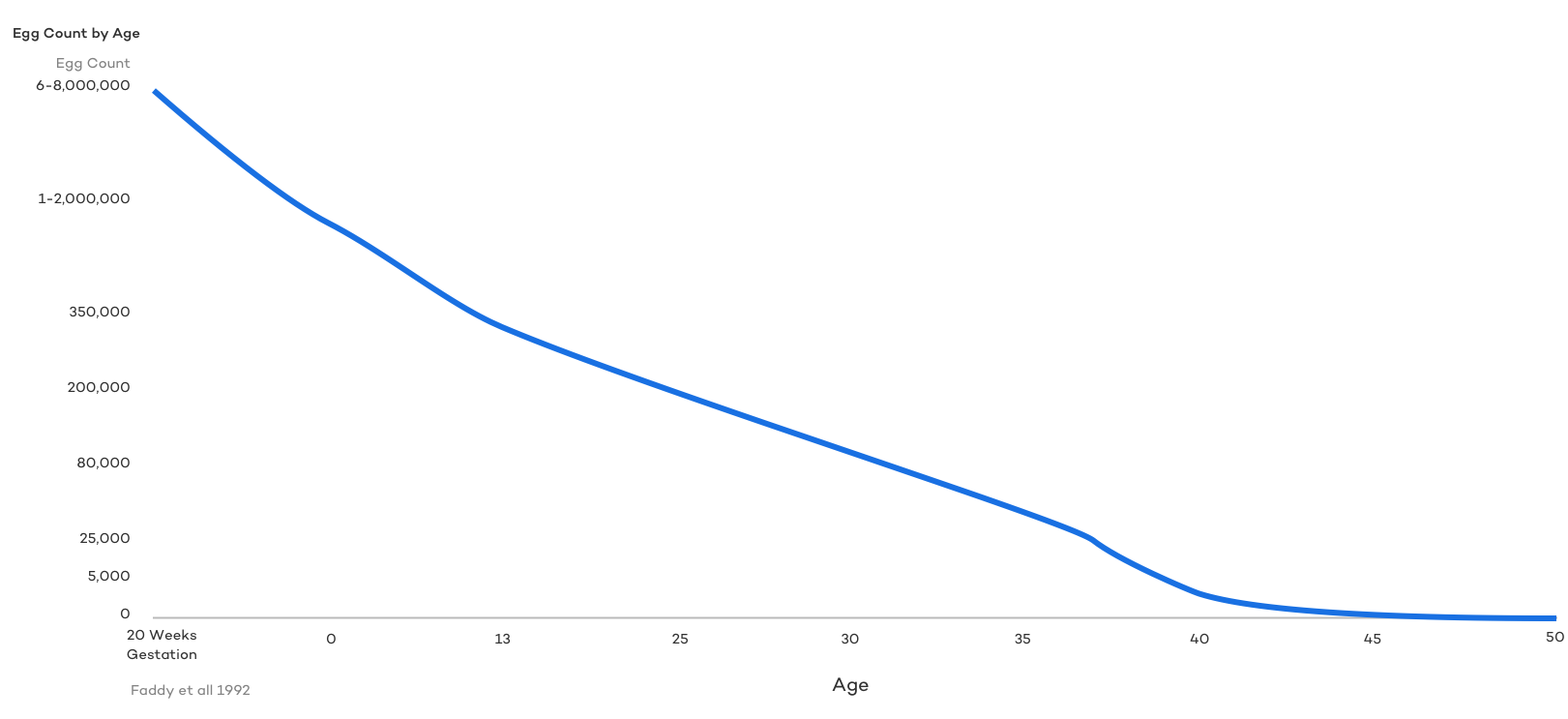
Declining ovarian reserve is an unavoidable consequence of normal aging in a woman. A woman’s ovarian reserve is actually at its peak before she’s even born. From this point on, it’s on the decline.
Around age 35-37, egg reserve takes a rather serious nosedive. At age 40, ovarian reserve is considerably low and by the early to mid 40s, most women only have about 5,000 eggs in reserve. By comparison, a healthy 25-year old can have over 100,000+ eggs in reserve.
Doctors measure ovarian reserve with a simple blood test called the Anti-Müllerian Hormone (or AMH) test. AMH is a hormone that’s produced by the cells inside a woman’s follicles. Eggs mature inside the follicle until they are eventually mature enough to be released during ovulation. Therefore, the number of follicles a woman directly correlates to the number of eggs “on deck,” and the level of AMH created by these follicles reflects that reserve. The higher your AMH level, the more eggs you have in reserve, the lower your AMH, the lower your egg count.
While egg count varies widely from woman to woman, declining egg quality is a foregone conclusion and well documented in women as they age.
When to Seek Help if you’re not getting pregnant?
Under 35
Heterosexual couples where the woman is under the age of 35 should consider seeking help if they are unsuccessful after 12 months of regular, unprotected sex.
Over 35
If the woman is over the age of 35 and has been unsuccessfully trying to conceive for six months, it’s time to get help. If you’re over 40, you should seek out a reproductive endocrinologist right away.
Exceptions
And, of course, single parents, LGBTQ or trans couples, or anyone with a diagnosis that may adversely affect fertility the earlier you seek help, the better. Earlier treatment can mean more options.
Diagnoses Known to Affect Fertility:
If you’ve already been diagnosed with a medical issue that’s known to affect fertility, or if you have a previous history of difficulties with fertility, consider seeking assistance right away. Conditions that can affect fertility include:
- Infrequent or absent menstrual cycle
- A hormonal imbalance, particularly low testosterone
- Polycystic Ovarian Syndrome (PCOS)
- A history of endometriosis
- A diagnosis of cancer or other condition whose treatment could affect fertility
- A history of serious infections, particularly sexually transmitted infections (STI)
- Pelvic Inflammatory Disease
- Having two or more miscarriages
- Having three or more abortions
- Erectile dysfunction that impedes your ability to have intercourse
- The inability to ejaculate
- Endocrine system disorders
- A history of organ transplants for either partner
- Known genetic disorders that may affect fertility
- Family history of premature menopause or premature ovarian failure
Basic Fertility Testing when You’re Not Getting Pregnant:
Once you’ve decided it’s time to seek help from a fertility specialist, you might wonder what kind of testing is used to assess your and your partner’s ability to conceive. Given that sperm make up half the genetics of a growing embryo and future child, it’s very important that both partners be tested so that your doctor can best guide your treatment.
Male:
The most important component of male fertility testing is the semen analysis. A semen analysis looks to confirm the presence of sperm in the semen and check three main attributes of the sperm:
- Sperm Count (number of sperm)
- Morphology (shape and appearance)
- Motility (movement)
A complete semen analysis will also measure:
- Volume
- pH (level of acidity)
- Progression (motion and forward progress)
- Semen viscosity (consistency)
- The presence or absence of white, red blood cells, or immature sperm
If the male’s results are not within normal parameters, your doctor may repeat the test or order additional blood work to check various hormone levels. It’s important to note that even in a fertile man, semen analysis results can vary widely from sample to sample. It may be necessary to have several analyses performed to get an accurate picture.
Female:
Female fertility testing involves answering a series of questions about your medical history, the regularity of periods, bloodwork to test hormone levels and for certain antibodies, and a transvaginal ultrasound to take a look at your ovaries and other reproductive organs. Depending on your history and what your doctor finds, he or she may also recommend a Hysterosalpingogram/Saline Sonohysterogram or a Hysteroscopy/Laparoscopy to more closely check the condition of your fallopian tubes and uterus. In order for conception to occur, your tubes must be healthy and open. Scar tissue, fibroids, or polyps in your uterus can impact implantation and change the shape of your uterus. It’s important to remember that there’s not just one test that can evaluate every variable involved in fertility.
Getting Pregnant with Fertility Treatments
Depending on your test results and age, most fertility doctors will recommend starting with the least invasive, most natural treatment possible. As general categories, the three starting options for fertility treatment are Ovulation Induction, Intrauterine Insemination (IUI), and In Vitro Fertilization (IVF).
Ovulation Induction
For women who have infrequent, irregular, or absent menstrual cycles (also known as anovulation), ovulation induction may be necessary to achieve pregnancy because eggs are released infrequently or not at all. Ovulation induction uses ultrasound and blood work monitoring in conjunction with hormone medications that stimulate egg development and ovulation. Once a follicle reaches maturity, an injection of human chorionic gonadotropin (HCG) and or Lupron is used to induce ovulation. After the shot, couples are then told to have timed intercourse during the next 36-40 hours. Ovulation induction can also be used in conjunction with IUI. By triggering your ovulation with medication, your doctor can help ensure ovulation takes place and calculate exactly when it will happen so that intercourse or IUI can be timed accordingly.
Couples starting with ovulation induction should ideally both be under 30 years of age, have normal anatomy of the uterus and fallopian tubes, and a normal sperm analysis. The best candidates are women whose ovaries are not working properly but who are otherwise healthy. For couples with unexplained infertility, ovulation induction can help the woman produce extra eggs, thus improving her odds of conceiving.
Intrauterine Insemination (IUI)
IUI is primarily a facilitator of natural conception. The goal of IUI is to increase the number of sperm that reach the fallopian tubes and subsequently increase the chance of fertilization. IUI provides sperm with a head start in that they don’t have to travel from the vagina and through the cervix, but it still requires a sperm to reach and fertilize the egg on its own. Sperm is collected, concentrated, and deposited into a woman’s uterus using a catheter. IUI can be used with women who ovulate normally as well as women who don’t. And it can be used with medication and without as long as there’s adequate sperm from a partner or donor and tends to be a bit more successful than ovulation induction on its own. IUI generally has a success rate of around 10-20% per cycle, but it becomes a less successful treatment option as patients get older. If IUI is going to work, it usually happens in the first few cycles of treatment .
IUI is typically not recommended for patients with fallopian tubes that are completely blocked, partially blocked, or open but diseased. In these cases, conception is challenging and can result in an ectopic pregnancy. If the male partner has a low sperm count (e.g., less than 10 million motile sperm) or decreased motility or the couple has been attempting to conceive for a long time with a male partner who has a normal semen analysis, IUI is usually not the first treatment of choice.
In Vitro Fertilization (IVF)
The third and most effective treatment option is IVF. During IVF, an egg retrieval is performed to remove eggs from a woman’s ovaries, which are then fertilized with sperm from a partner or donor in a laboratory. After the embryos are allowed to grow for 3-5 days, one embryo (but occasionally two) is subsequently transferred back into the woman’s uterus during an embryo transfer. IVF is used in conjunction with many different medication protocols to produce more eggs, higher quality embryos, and improve the uterine lining for implantation.
IVF is the most effective fertility treatment available. Success rates vary significantly depending on the mother’s age, with younger patients generally achieving better results. CDC data indicates IVF has an average success rate of 27.3% and results in live births 22.2% of the time. These numbers depend on many variables, including age, embryo quality, sperm and egg quality, infertility diagnosis, and the clinic performing treatment. For those under 35 the prognosis is about twice as good as the average with success rates around and in many cases, over 50%. The CDC offers an IVF Success Calculator for parents who want to understand their chances of conceiving based on age, height, weight, infertility diagnosis, and other health factors.
IVF is so successful because it removes so many female and male fertility barriers from the process. Because conception is actually occurring in a laboratory and an already fertilized egg is being placed into the uterus, issues with the cervix or fallopian tubes become irrelevant. A woman with completely blocked fallopian tubes can still conceive with IVF. The same is true of nearly all-male factor infertility problems that make it difficult or impossible for sperm to reach the fallopian tubes to fertilize the egg. By combining IVF with Intracytoplasmic Sperm Injection (ICSI) to inject a single, healthy sperm into an egg, IVF overcomes any obstacles resulting from abnormal sperm quality, movement, or shape.
Reproductive Immunology
Reproductive Immunology is a field of medicine that studies the interactions between the immune system and the reproductive system. It is believed that the immune system plays a major role in recurrent pregnancy loss and repeated IVF failures. Fertility specialists believe the immune system may react to an embryo as an “invader” and thus attempt to stop the growth of these cells. Many treatments are being utilized in the field of reproductive medicine to reduce inflammation and suppress the immune system to support successful pregnancy outcomes. Women who have a history of failed IVF or recurrent pregnancy loss should be tested for biomarkers of inflammation in their blood and endometrial tissue. Since high carb/low-fat diets are also believed to contribute to higher levels of inflammation throughout the body, CNY Fertility recommends a ketogenic fertility diet that is high in fat, moderate, and proteins and eliminates carbs (including sugars, fruits, vegetables, and fiber). Other pharmacologic treatments can also be helpful in reducing inflammation.
Donor Eggs/Sperm
When sperm or egg quality are believed to be the cause of infertility, using donor eggs or donor sperm is a possibility to help get pregnant. Egg quality is one of the major reasons pregnancy rates go down in older women, and miscarriage rates go up. For older women, using their own eggs may not allow them to get pregnant. When this is the case, donor egg IVF may be recommended.
While Intracytoplasmic Sperm Injection (ICSI) or ICSI combined with sperm extraction can solve most male factor fertility issues, there are still times when donor sperm may be necessary, such as the case with same-sex female couples, single mothers, couples where the male is a carrier of a genetic defect, or failed fertilization with ICSI. Donor sperm can be used for IUI, IVF, or reciprocal IVF.
Gestational Surrogacy
Surrogacy is an ideal option for women who have had a hysterectomy, endometrial ablation, Asherman’s Syndrome and can not get pregnant but still want to have a child. Women who’ve experienced numerous miscarriages with unsuccessful immunological treatment may also consider using a gestational carrier, along with women who have preexisting medical conditions like diabetes or a heart condition that make pregnancy dangerous or those who have a non-functioning uterus. Same-sex male couples or single fathers will also need to use a surrogate to have a child of their own.
Surgical Considerations
At any time during treatment– before, during, or after IVF, Reproductive Immunology, or using Donor Eggs/Sperm, it may be advised to have surgery to diagnose and treat certain conditions surgically.
- Laparoscopy: A laparoscopy is frequently recommended when endometriosis, fibroids, or polyps are suspected, or pelvic pain is reported. By inserting a small camera into the abdomen, a surgeon is able to visualize the abdominal and pelvic organs, including the outside of the uterus, fallopian tubes, and ovaries. He or she is able to check for overall health, confirm the diagnosis, and in many cases, remove, repair, or treat the problem during the same procedure.
- Hysteroscopy: A diagnostic hysteroscopy can be performed concurrently with a laparoscopy and is used to view the inside of the uterine cavity and determine the source of any abnormal uterine bleeding and remove any uterine growths.
- Ovarian Drilling: For women with PCOS who are not able to ovulate even with the use of fertility drugs, ovarian drilling may be recommended. It involves making three to eight tiny punctures into the ovaries. Doing so may allow you to ovulate on your own or make you more receptive to treatment protocols.
Tubal Surgeries
When a blockage in the fallopian tube is preventing egg and sperm from meeting and/or an embryo from moving into the uterus to implant, surgery may be recommended to confirm and correct the problem. Some common tubal procedures include:
- Tubal Ligation Reversal: After an elective tubal ligation, this surgery reconnects the ends of the fallopian tubes, effectively reversing the surgery and restoring fertility.
- Salpingectomy: Occasionally, there is a build-up of fluid in the fallopian tube (called hydrosalpinx) that makes it difficult for a woman to conceive. It may be necessary to remove the portion of the tube that generates the fluid. Alternatively, sometimes the surgeon will elect to surgically create a new opening in the tube closest to the ovary during a salpingostomy
- Fimbrioplasty: The little fingers at the end of the fallopian tube (fimbria) that help to sweep the egg into the tubes can sometimes become damaged, scarred, or blocked. A fimbrioplasty uses microsurgery to clear any scar tissue, remove any blockages, and reconstruct the fimbria.
- Selective Tubal Cannulation: When the portion of the tube closest to the uterus is blocked (called a proximal tubal obstruction), a surgeon can use a catheter covered wire guided by ultrasound or x-ray through the cervix, into the uterus, and into the fallopian tube to surgically open the tube(s). The blocked region is opened up using a balloon device at the end of the catheter.
Pregnancy Loss
If you’ve been able to successfully conceive but not carry to term, it’s important to determine what is going wrong in the chain of events. While miscarriage is quite common and frequently happens due to genetic abnormalities in the embryo that don’t allow it to survive, recurrent miscarriage is not. Around 1% of women experience recurrent miscarriage. Doctors define this as two or more miscarriages in a row. Women who experience recurrent pregnancy loss are advised to be tested for blood clotting disorders, thyroid or uterine problems, and/or chromosomal abnormalities that parents may be passing to the embryo.
The Bottom Line About Getting Pregnant
Conception is an overwhelmingly complex process that most people take for granted. When you dig into the details and begin to understand everything involved in getting pregnant, you can see how many places there are for things to go awry.
It’s generally recommended that people try to get pregnant on their own for 6-12 months unless diagnosed with a condition that is known to cause infertility. Fortunately, when getting pregnant naturally isn’t going as planned, medical science has figured out ways to bypass many of the fertility problems experienced by both women and men. From medications to surgical interventions and traditional fertility treatments like IUI and IVF, there’s bound to be a solution that can help you get pregnant.
If you feel like something isn’t going right for you, it’s best to trust your gut instinct and set up a consultation with fertility specialists who can help you get pregnant and become the parents you want to be!