Clomid vs Letrozole for Fertility

For over 50 years, Clomid has been the most commonly prescribed oral fertility medication. It remains a first-line treatment for women struggling with infertility, especially those with ovulatory disorders such as polycystic ovary syndrome (PCOS)
Letrozole (Femara) was originally approved by the FDA for treating estrogen receptor–positive breast cancer. Over time, it has also become widely used off-label in fertility care. Today, it is considered a highly effective alternative to Clomid for ovulation induction.
With both medications widely prescribed, research has focused heavily on comparing the effectiveness and clinical outcomes of both medications.
In this article, we’ll review the evidence comparing Clomid vs. Letrozole and examine which option is emerging as the preferred first-line treatment.
Fast Facts
- Mechanism: Both Clomiphene (Clomid) and Letrozole (Femara) lower estrogen levels. This signals the body to produce more FSH and LH, the hormones that stimulate follicle development and trigger ovulation.
- Effectiveness: Both medications significantly increase the chances of ovulation and pregnancy.
- Treatment Options: Clomid and Letrozole can be used with timed intercourse cycles, intrauterine insemination (IUI), and in vitro fertilization (IVF).
- Research Findings: Most studies suggest that Letrozole is slightly more effective than Clomid at inducing ovulation and supporting pregnancy..
- Clomid Resistance: Letrozole is frequently prescribed for patients who do not respond to Clomid.
- Male Fertility: Both medications are also used to treat male infertility related to low testosterone.

What are Clomid (Clomiphene Citrate) and Letrozole (Femara)
Clomid and Letrozole are oral medications that stimulate the ovaries to develop and release mature oocytes (eggs).
They work by lowering estrogen levels, which the hypothalamus interprets as a signal to increase production of FSH and LH. These hormones, especially FSH, stimulate follicle growth, oocyte development, and ovulation (the release of the egg).
In short, both medications improve fertility in two key ways:
- Increasing the number of mature, high-quality oocytes developed each cycle
- Inducing ovulation
How Clomid and Letrozole Work
As mentioned, Clomid and Letrozole’s primary effect is “reducing” estrogen levels. How these medications reduce estrogen levels is the primary difference between these two medications.
Clomid Mechanism of Function
Clomid is a selective estrogen receptor modulator, meaning it blocks estrogen receptors in the brain. By blocking estrogen receptors, the brain is tricked into believing there are low levels of estrogen, which again triggers the pituitary to make more FSH and LH.
The amount of time Clomiphene is in the body is approximately 2 weeks (which is significantly longer than Letrozole). Clomiphene’s prolonged half-life causes a blocking of estrogen receptors and increases FSH/LH production for a significant length of time after the medication is stopped.
Clomid’s prolonged effects on FSH and estrogen production cause bilateral follicular growth–more than would be expected when compared to a natural cycle.
Letrozole Mechanism of Function
Letrozole is a nonsteroidal aromatase inhibitor, meaning it blocks the conversion of androgens into estrogen. As a result, Letrozole directly lowers estrogen levels in the body.
With less circulating estrogen, the brain responds by increasing FSH and LH production.

Clomid vs. Letrozole for Inducing Ovulation
Ovulatory disorders are one of the most common causes of infertility. They affect approximately 30-40% of infertile women. Polycystic Ovarian Syndrome (PCOS) is the most common cause of anovulatory infertility and also the most common diagnosis of infertility in general.
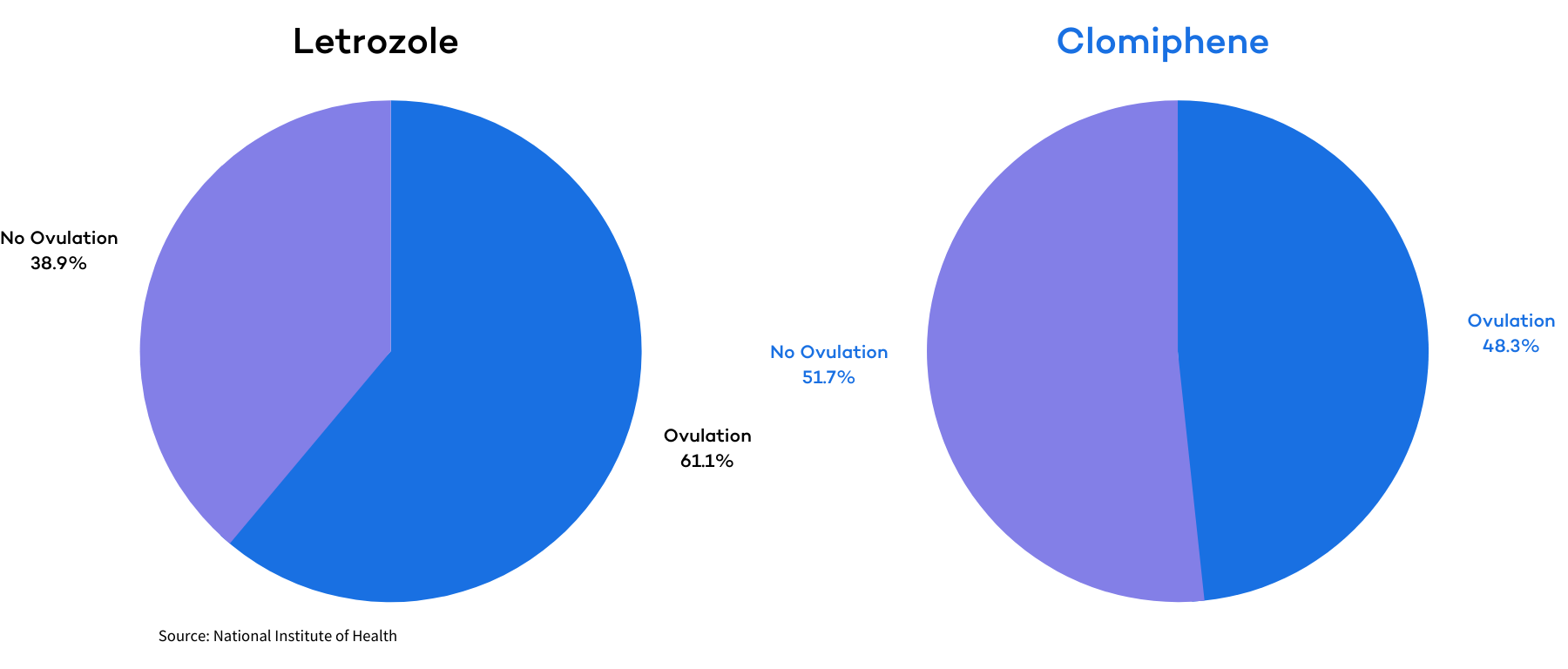
In 2014, the National Institute of Health (NIH) published a study that measured the effectiveness of Letrozole and Clomid in patients diagnosed with PCOS .
The study included 750 women: 374 who received Letrozole and 376 who received Clomiphene. Both groups received the meditations for 5 days, starting on day 3 of their cycle, for up to 5 cycles.
The women in the Letrozole group had a cumulative ovulation rate of 61.7% (834 times in 1352 cycles). The women in the clomiphene group ovulated 48.3% of the time (688 times in 1425 cycles).
Other studies have shown similar results.
The research, however, is not entirely one-sided. A 2020 study of anovulatory women with PCOS also compared Letrozole and Clomid for ovulation induction. Ovulation rates were similar—86.7% for Letrozole and 85.2% for Clomid.
Despite this, researchers concluded that Letrozole was the better option because it was associated with higher pregnancy rates, shorter time to conception, and a lower risk of multiple pregnancies due to more frequent mono-follicular growth.
Clomid Resistance
Clomid may induce ovulation in many patients, but it is not effective for everyone. If ovulation does not occur, a doctor may increase the dosage. When higher doses still fail, the patient is considered Clomid resistant.
There are several reasons why Clomid resistance may occur. The most common are in women with a body mass index (BMI) over 25.as well as those with an elevated prolactin level. Women with PCOS are the most common to experience Clomid resistance, especially those who are diagnosed with insulin resistance or with hyperandrogenic levels.
Research has shown that Letrozole can help to induce ovulation for some women who have previously failed with Clomid or are considered “Clomid Resistant.”
In one study, Letrozole significantly improved ovulation rates and live birth rates for women who failed to ovulate with Clomid.
Clomid vs. Letrozole Pregnancy & Live Birth Rates – PCOS
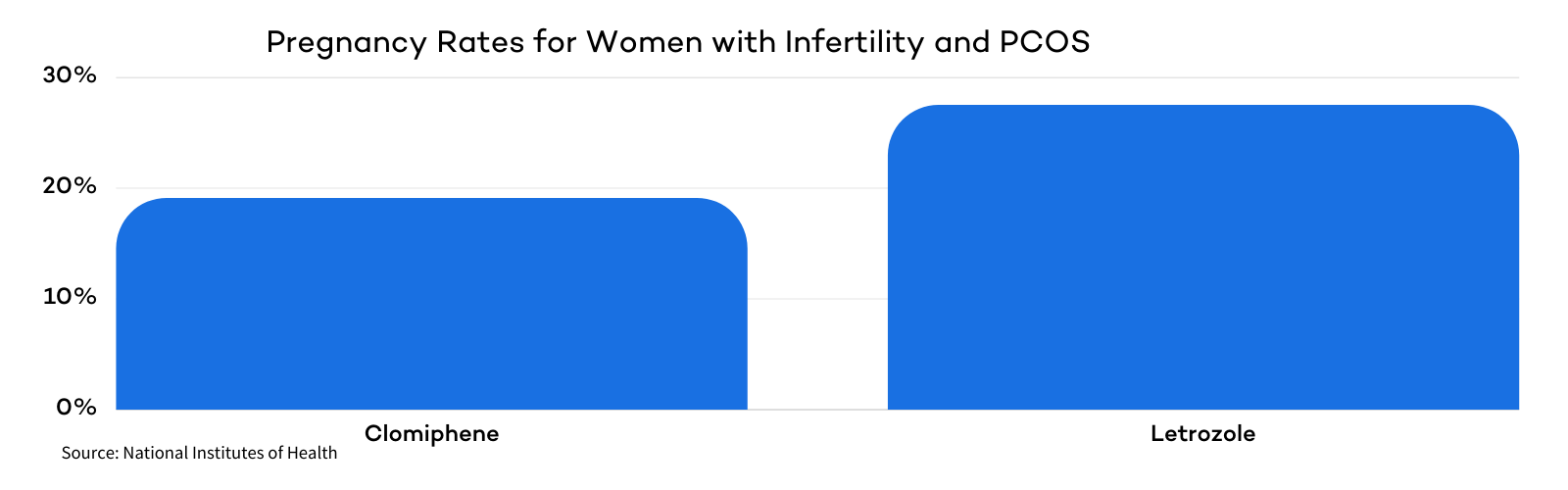
In the 2014 NIH study mentioned above, Letrozole was more effective at inducing ovulation for patients with Polycystic Ovarian Syndrome (PCOS).
In that same study, researchers also measured the effects of Clomid and Letrozole on live birth rates. Of the 374 women treated with Letrozole, 103 (27.5%) had a live birth. Of the 376 women treated with Clomiphene, only 72 (19.1%) had a live birth.
In another study, researchers compared the effects of Letrozole and Clomiphene as first-line ovulation induction drugs to treat infertile PCOS women.
They split 103 infertile women with PCOS into Clomiphene and Letrozole treatment groups. The patients treated with Letrozole experienced a pregnancy rate nearly three times that of the Clomiphene group.
The pregnancy rates were 21.56% for the Letrozole group and 7.84% for the Clomiphene group.
Clomid vs. Letrozole Pregnancy & Live Birth Rates – Unexplained Infertility
Both Clomid and Letrozole can help women with unexplained infertility achieve pregnancy. However, there is no clear consensus on which is most effective.
Studies have produced conflicting results, with some supporting Clomid and others favoring Letrozole. Overall, most studies show that the two medications yield pregnancy and live birth rates that are statistically similar in this group of patients.
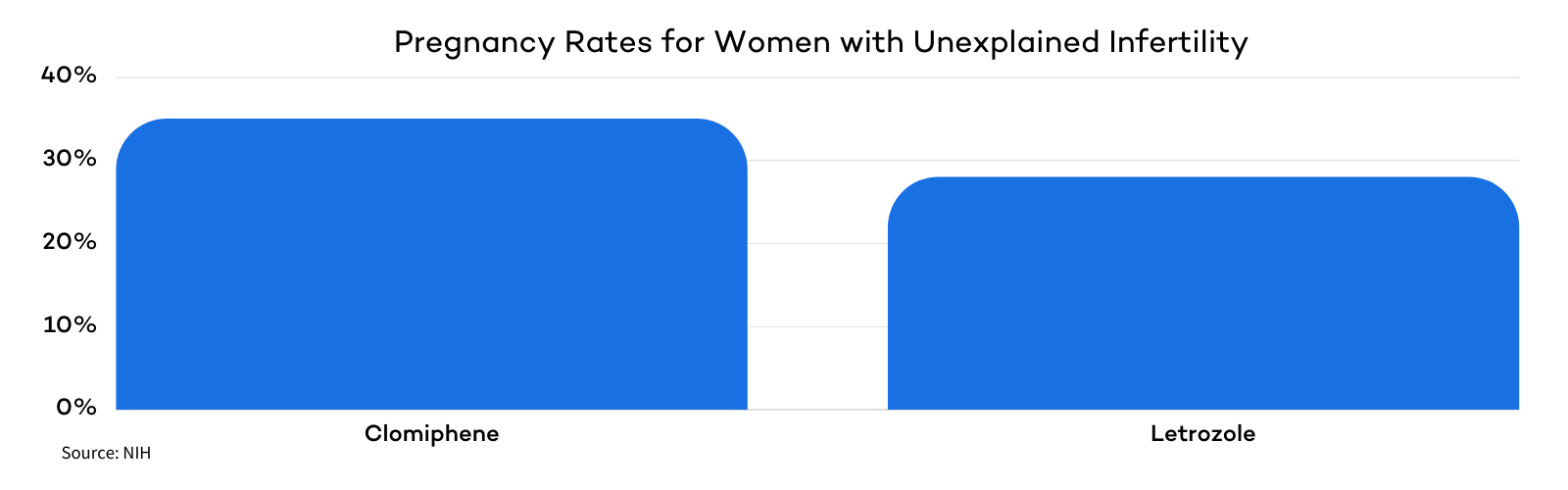
Following the 2014 National Institutes of Health (NIH) study showing that Letrozole outperformed Clomiphene for women with PCOS, the NIH also examined their effectiveness in treating unexplained infertility.
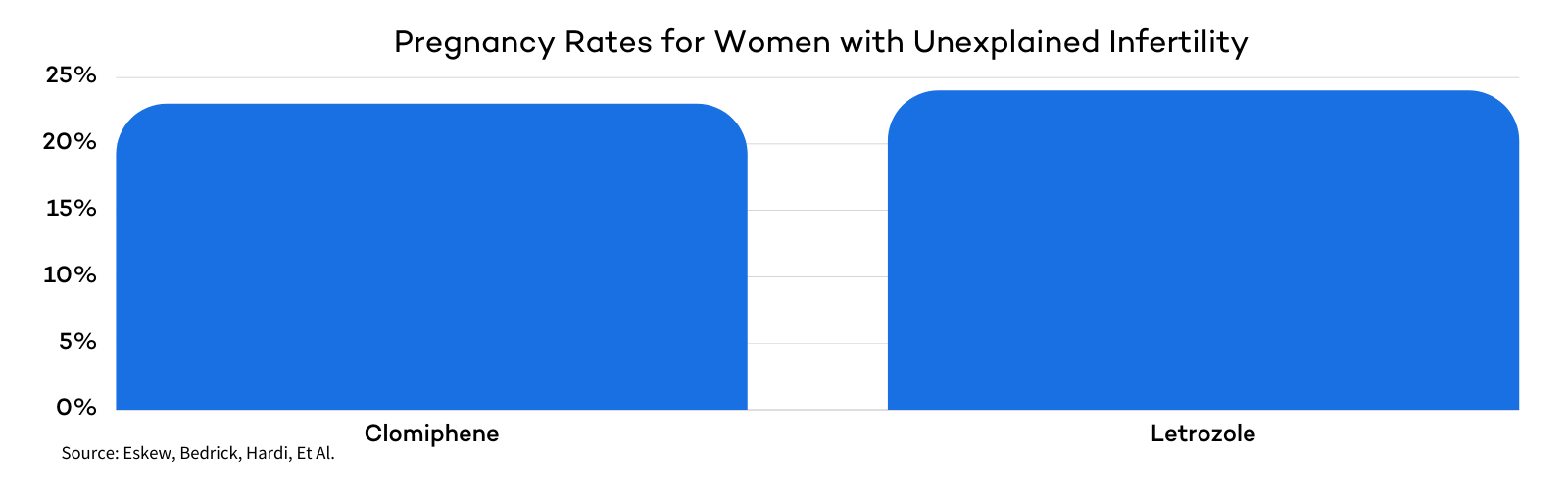
One trial, published in the New England Journal of Medicine (2015), compared the two drugs in women undergoing timed intrauterine inseminations (IUI) for up to four cycles. The results showed pregnancy in 35% of women taking Clomiphene and 28% of women taking Letrozole.
While pregnancy rates differed, live birth outcomes were similar: 23% of women in the Clomiphene group achieved live births compared with 19% in the Letrozole group.
Although the Letrozole group showed slightly lower results, the difference was not statistically significant. Researchers concluded that Clomiphene is as effective as Letrozole for treating unexplained infertility.
Another study also compared Clomiphene and Letrozole in women with unexplained infertility. The randomized controlled trial found that Letrozole may improve implantation and pregnancy outcomes.
In this study, 23.1% of women treated with Letrozole conceived, compared with 10.7% in the Clomiphene group.
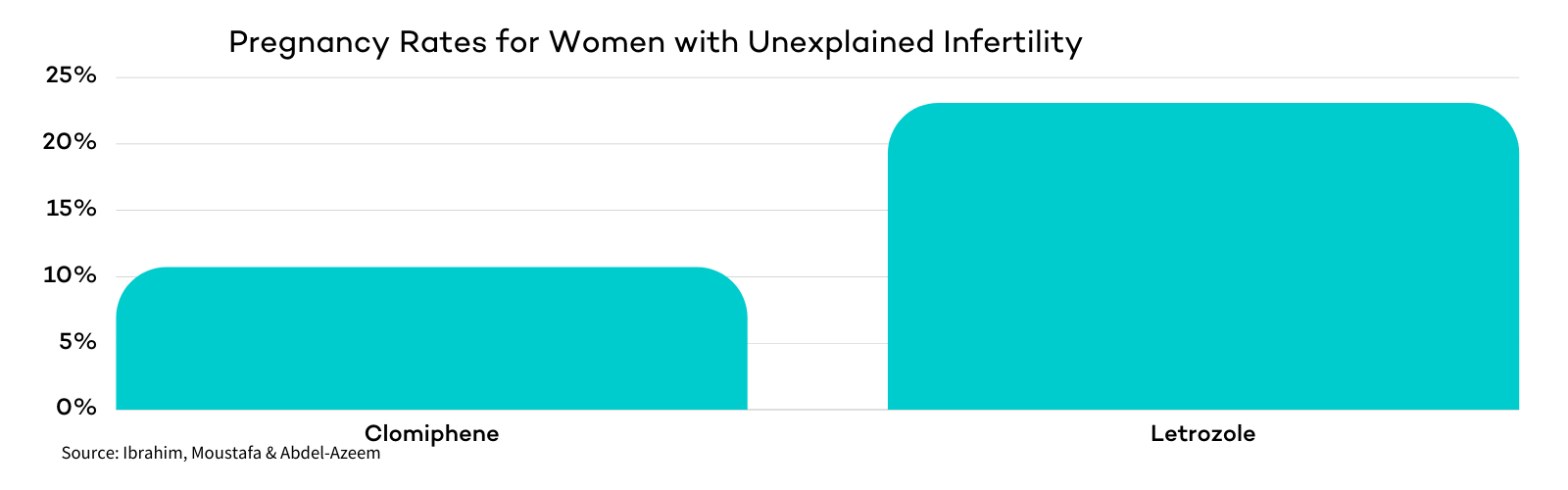
In addition to higher pregnancy rates, women treated with Letrozole also demonstrated a statistically significant improvement in endometrial receptivity.
Researchers concluded that Letrozole has a more favorable effect on the uterine lining compared to Clomiphene, which may help explain its potential to improve implantation and pregnancy outcomes.
A 2019 systematic review and meta-analysis evaluated data from 8 randomized controlled trials comparing Letrozole and Clomiphene in patients with unexplained infertility.
The analysis found that 24% of patients treated with Letrozole and 23% of those treated with Clomiphene achieved pregnancy. There was no significant difference between the two groups in either pregnancy rates or live birth rates.
Researchers concluded that there is no significant statistical difference in the effectiveness of Clomid or Letrozole to improve clinical outcomes.
Differences in Side Effects That Impact Fertility
One of the main reasons fertility specialists increasingly prescribe Letrozole is its lower risk of side effects compared to Clomiphene.
Clomiphene can lead to a thinner endometrial lining and a higher likelihood of multiple pregnancies in some patients.
These differences are thought to stem from the distinct mechanisms of action of each medication and the duration of their activity in the body.
Endometrial Thinning
Some women develop a thin uterine lining (endometrium) when using clomid for ovulation induction. A thin lining reduces implantation rates and chances of pregnancy.
Researchers believe this effect is due to Clomid’s prolonged action on estrogen receptors in the uterus. In a natural cycle, estrogen stimulates the endometrium to thicken. But because Clomid blocks estrogen receptors not only in the brain but also in the uterus, the endometrium may fail to develop correctly.
Since Letrozole also lowers estrogen, it might seem logical that it would have the same effect. However, studies show that patients treated with Letrozole generally have thicker endometrial linings compared to those treated with Clomiphene.
This is likely because Letrozole is cleared from the body more quickly, allowing the uterine lining enough time to thicken.
Multiple Pregnancies
Both Letrozole and Clomid can produce more than one oocyte-containing follicle, which may result in a pregnancy of multiples. However, research indicates that Letrozole results in more mono-follicular cycles, reducing the risk of multiples.
Mono-follicular cycles lead to singular pregnancies (rather than twins and triplets) and are thus much safer for both mom and baby.
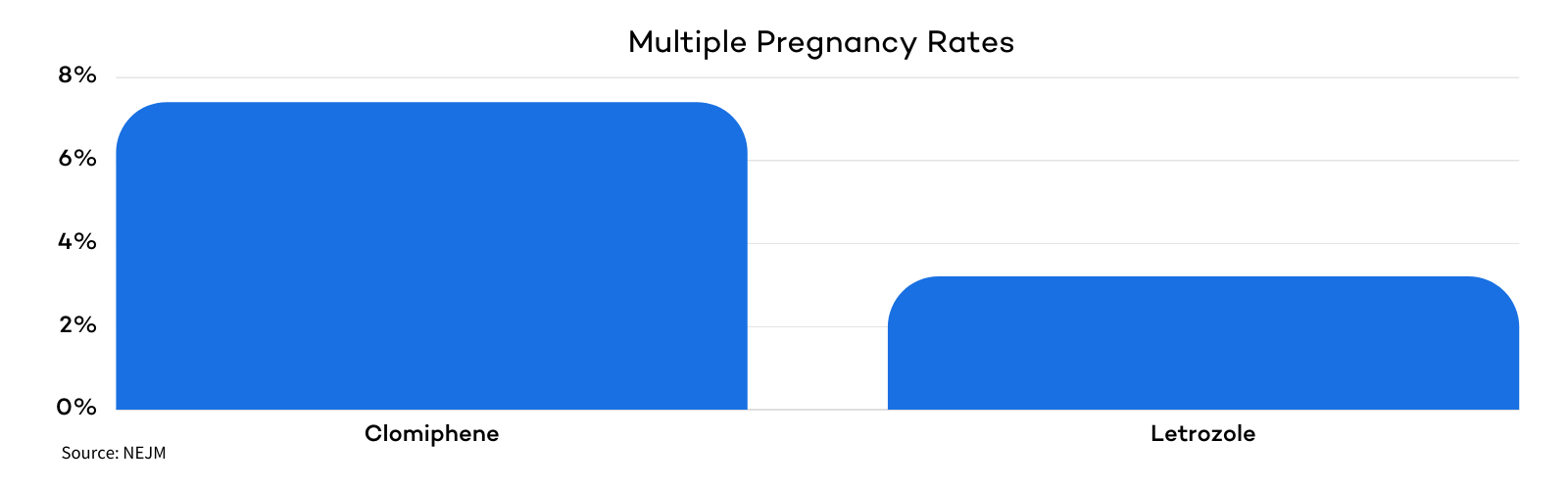
Letrozole has a shorter half-life than Clomid. During a Letrozole cycle, as the dominant follicle grows, it produces increasing amounts of estrogen. This estrogen is not blocked by Letrozole’s aromatase-inhibiting effect, which leads to suppression of FSH.
As a result, the smaller developing follicles stop growing. In most women, this process allows a single dominant follicle to mature, leading to a single oocyte ovulating rather than multiple.
In a Clomid cycle, FSH production is not suppressed by rising estrogen levels. The consistently high levels of FSH during a Clomid cycle cause multiple follicles to reach maturity.
Cost Comparison
Clomid and Letrozole are generally covered by insurance at similar rates and are comparably priced when paid out of pocket. According to GoodRx, Letrozole can cost as little as $20.50, while Clomiphene can be found for around $23.00.
Clomid vs. Letrozole: The Takeaway
Clomid and Letrozole are both well-established fertility medications. They reliably induce ovulation and increase egg production at a fraction of the cost of injectable gonadotropins. Both can also be used alongside a variety of fertility treatments to improve the chances of pregnancy.
While research findings are mixed, Letrozole generally appears more effective at inducing ovulation and improving pregnancy rates, particularly in women with PCOS. Many fertility specialists also prefer Letrozole because it is associated with fewer side effects.
As always, decisions regarding which fertility treatment is best for you should be made under the guidance of a doctor. Scheduling a consultation with one of our fertility specialists can help determine which medication is best suited to your individual needs and family-building goals.



